|
||||||||||||||||||||||||||
| ||||||||||||||||||||||||||
|
Case Study
| ||||||||||||||||||||||||||
Index
Interesting case submitted by Dr Jan Hnizdo of Prague
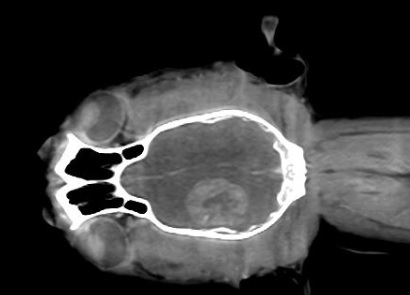
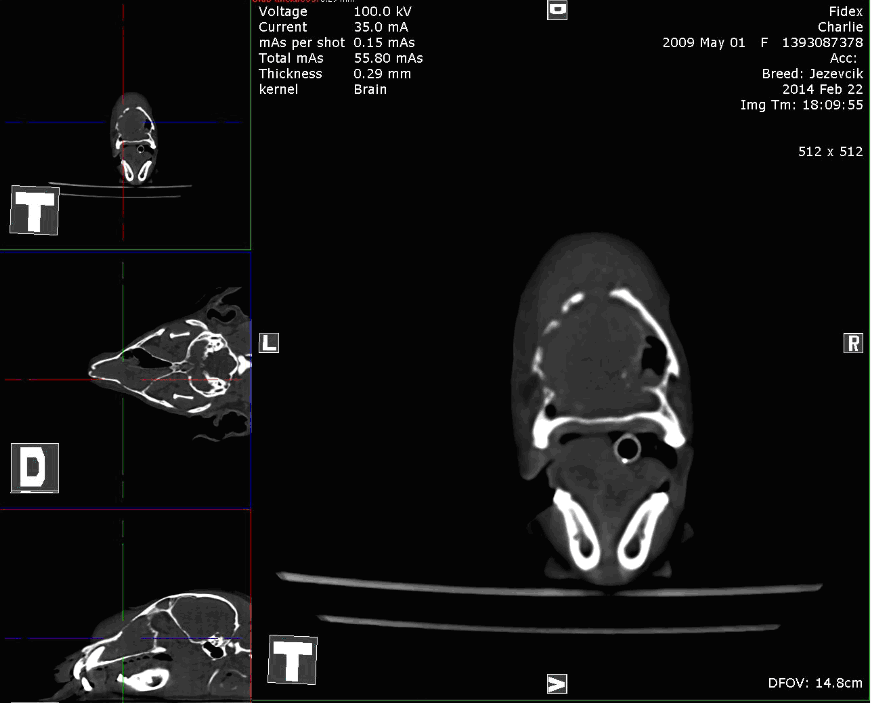
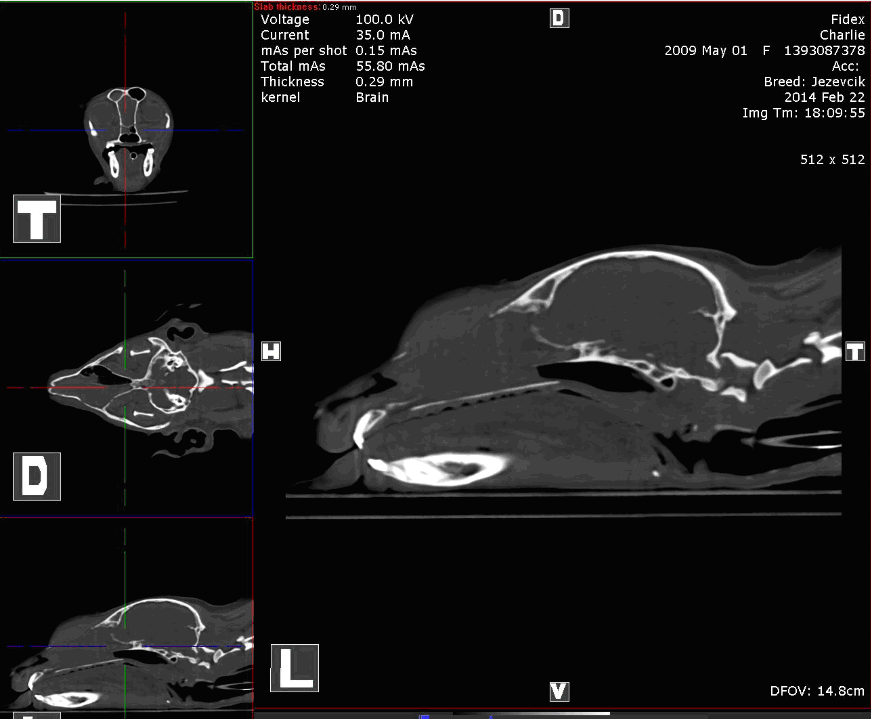
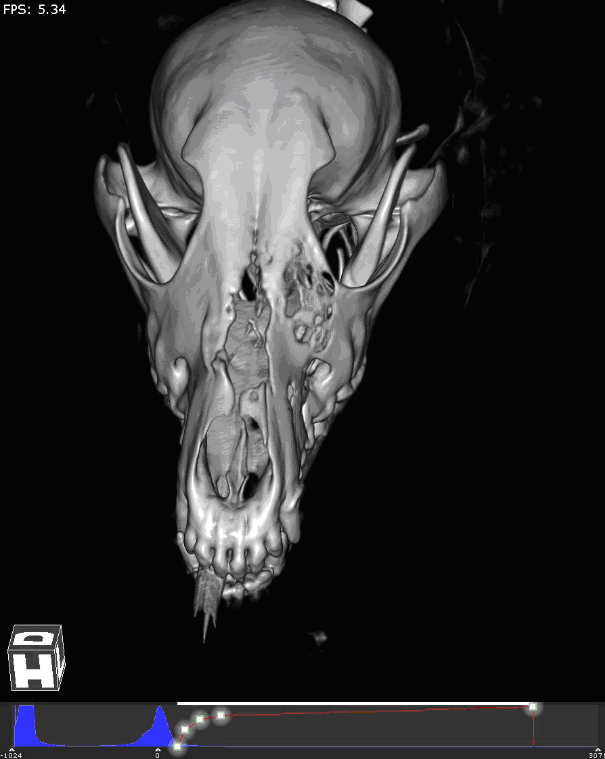
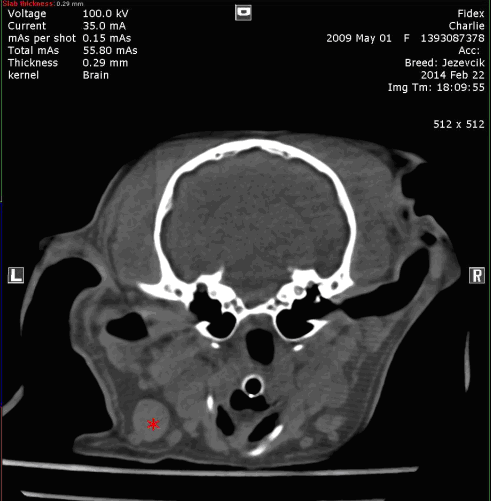
Brain tumor imaged with Fidex by Dr. Fred Sanspoux, Capveto Bellac Radiology review: CBCT scan of the skull, pre and post contrast, good image quality. Description: A bone resorption area around the tooth root of the incisor III on right maxillary arch. The remaining dental structures is usual appearance. The nasal cavities are normal. At the level of the brain, a mass intra-axial of diameter of 1.8 cm was noted in the left parietal lobe. This mass is well defined post contrast, certainly has a hypodense necrotic center. Mass effect is visible on the center line which is deflected to the right through almost all its length and on the left lateral ventricle which is compressed. The cerebellum seems still in place. The ears are normal. Retropharyngeal lymph nodes are normal. CONCLUSION:
Mild Nasal Stridor Patient: Cat, DSH, 13 years, indoor History: 7 months before admittance to our clinic the owner detected acute onset of unilateral nasal discharge, consequently was histologically confirmed nasal lymphoma; during diagnosis FeLV Snap test was positive; patient was treated by doxycyklin and recombinant interferone administering; nasal discharge disappeared, patient referred for further oncological treatment. Clinical examination: mild nasal stridor, otherwise normal (no nasal discharge, no peripheral lymphadenopathy). General bloodwork: inconclusive. PARR clonality of bioptate previously taken for histopathology confirmed B-cell lymphoma. PARR clonality of peripheral blood: heteroclonal (nonneoplastic) lymfocyte population. Abdominal USG: normal findings. CT of a head (contrast): bilateral nasal mass of soft tissue density detected (moderate contrast intake), severe damage of the nasal labyrinth, right sided deviation of the septum, osteolytic changes detected, crybroid and frontal sinuses appeared to be intact, severe periapical osteolytic changes around premolars and molars (accidental finding). CT of the thorax (contrast+breath holding): mild peribronchial infiltrate in a left caudal lung lobe (unknown significance and ethiology), no mediastinal lymphadenopathy. Diagnosis: Nasal B-cell lymphoma stage I. Conclusion: Lymphoma is the most common nasosinal type of tumor in cats. CT of the nasal cavity combined with rhinoscopically assisted or blind biopsies are essential tools which lead to the definitive diagnosis. After histopathological confirmation of lymphoma it is also very important to employ further examination processes such as immunohistochemical staining, PARR clonality analysis or flow cytometry to differentiate the subtype of tumor. This information has a prognostic relevancy and is very important for further therapeutic decision making. Precise patient staging is also very important for next management. Feline nasal lymphomas are described as a rare FeLV related. The relevancy of one positive snap test result in our case is not clear. Snap test for FeLV can unfortunately show a signficant amount of false positive and also false negative results. Radiotherapy as one of the most effective therapeutic options is the therapy of choice in nasal lymphoma cases in cats. Additional chemotherapy does not enhance the median survival time. In our case we can see very good response to the chosen therapeutic approach. Next staging include CT scanning will be provided after three months.
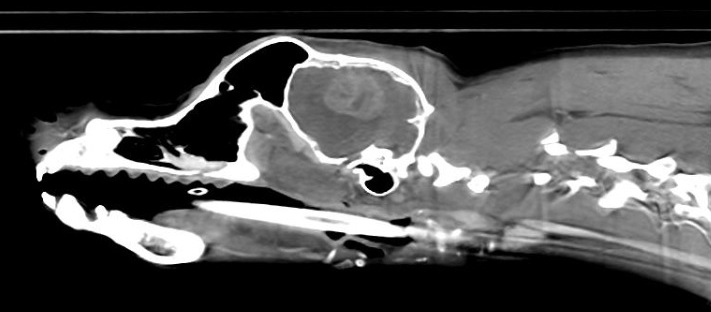
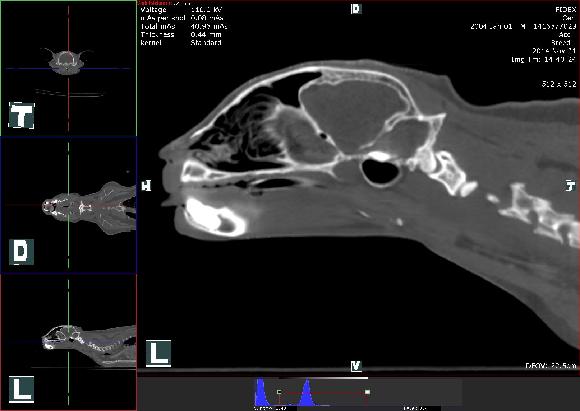
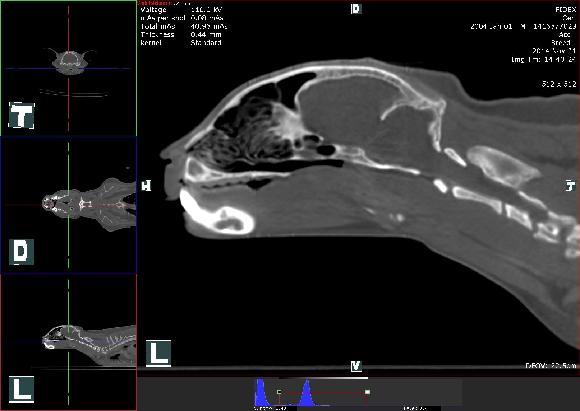
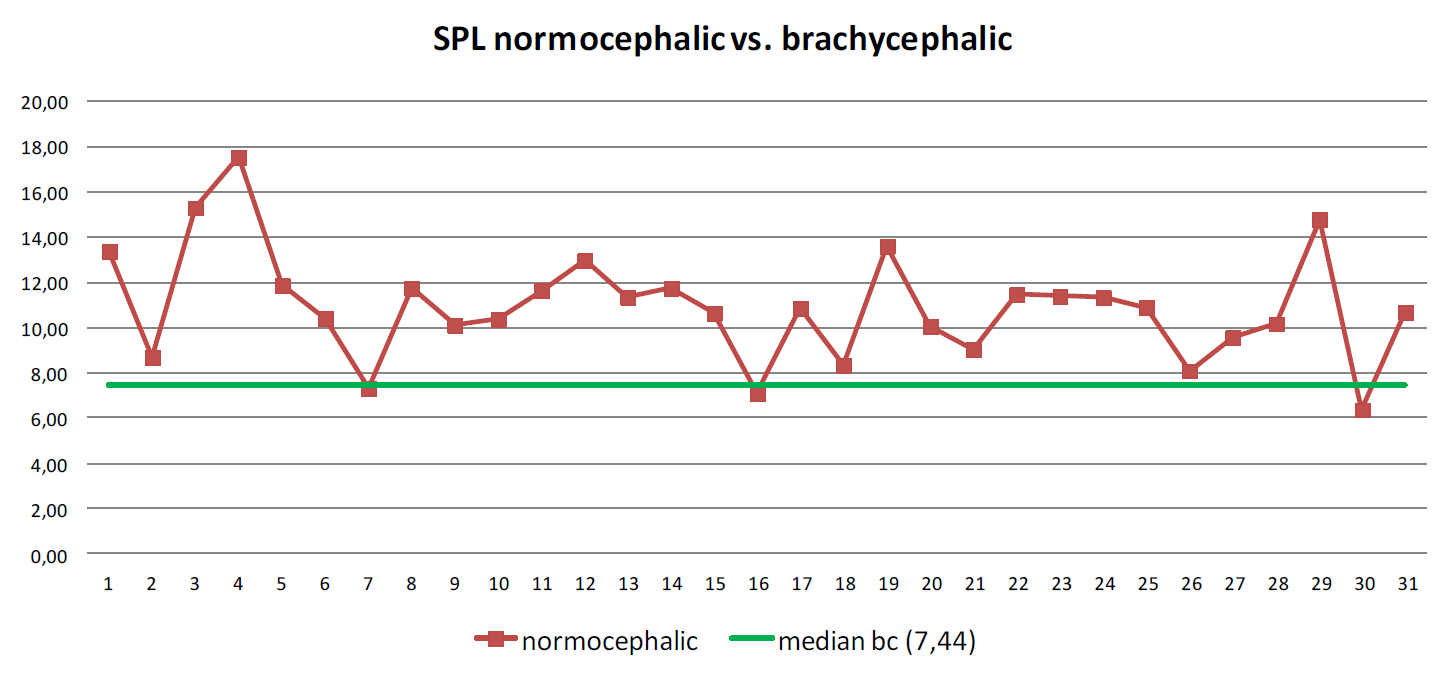
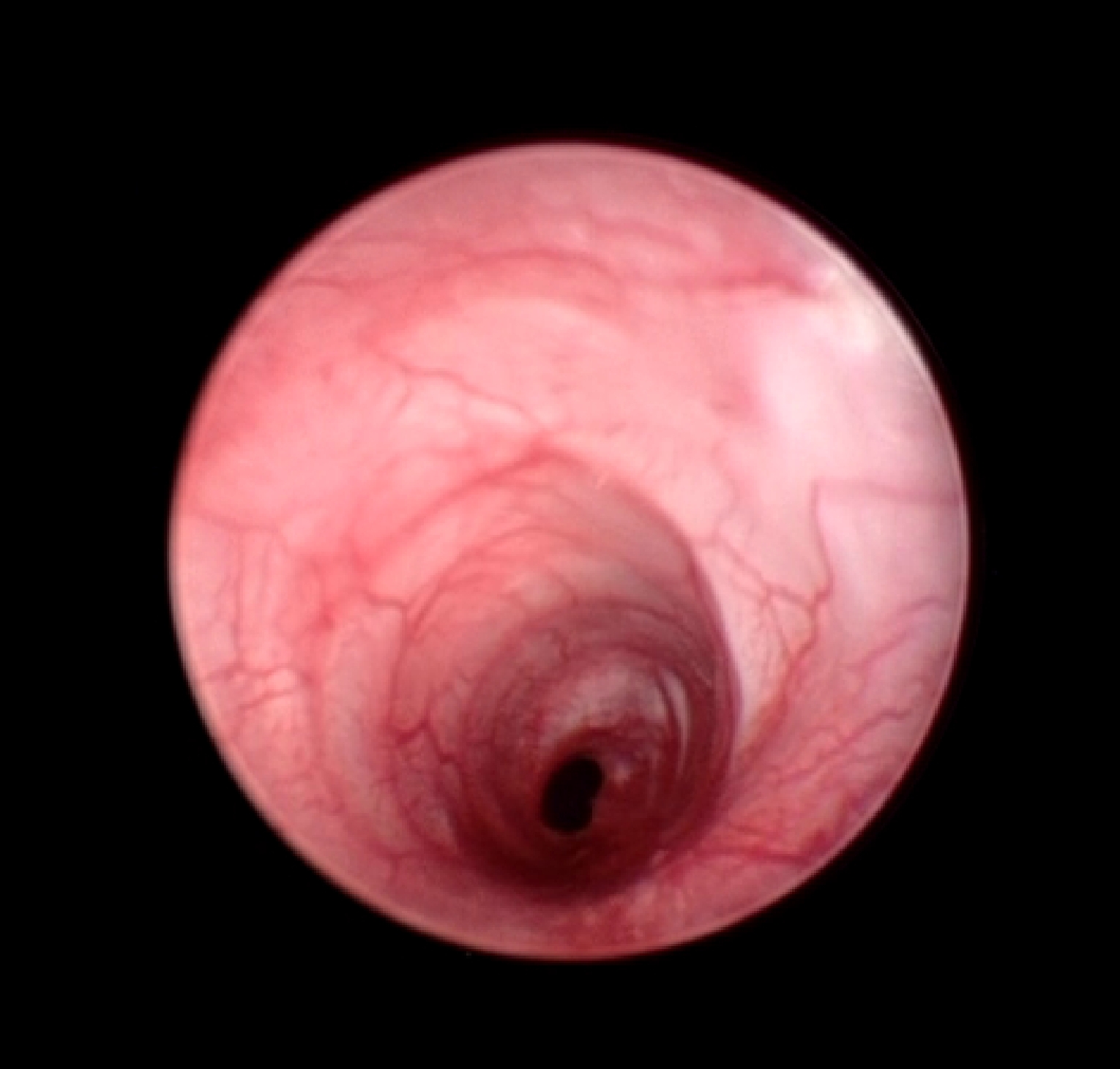
Use of Cone Beam CT for Objective Assessment of BOAS Summary: The goal of this study was to find an objective diagnostic approach in BOAS cases by using a combination of Cone Beam CT and endoscopic evaluation of the respiratory system in brachycephalic dogs. In the study were included 22 brachycephalic dogs and as a control group 31 normocephalic dogs. All brachycephalics had at least one of the BOAS symptoms. All patients underwent head and pharyngeal area computed tomography. All patients with brachycephalic syndrom were also endoscopically evaluated. The study looks for a correlation between the lenght and width of the soft palate relative to the meatus pharyngeus diameter and compares measurements in brachycephalic and normocephalic dogs. Preface: Brachycephalic dogs have very unique upper respiratory anatomy which in some cases can lead to upper airway obstruction.
The typical anatomic abnormalities are shortened skull, compressed nasal passage, stenotic nares, enlarged tonsils, elongated and
hypertrophic soft palate, everted laryngeal saccules, narrowed rima glottidis and collapse of the larynx and trachea.3 In most of these dogs a combination of
compressed and shortened structures of upper airway leeds to increased negative pressure on inspiration to adequate ventilation.
4,5 The primary components of BOAS are stenotic nares, elongated soft palate and hypoplastic trachea. Secondary components
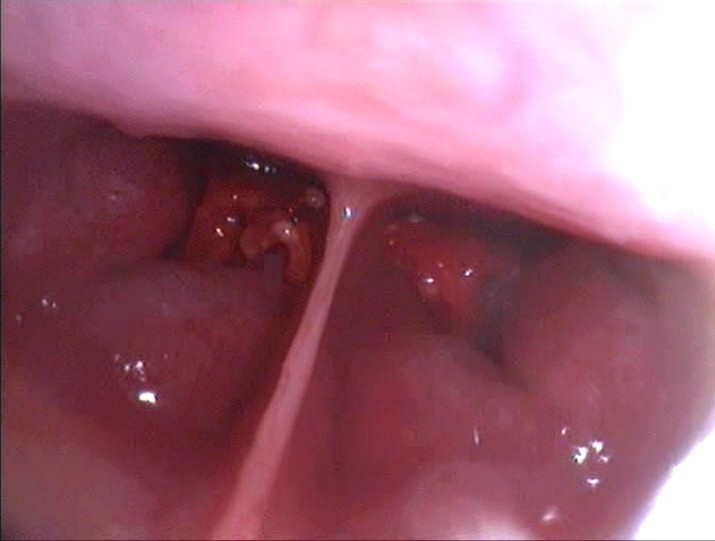
such as everted laryngeal saccules (Fig.1), soft palate thickening, laryngeal collapse and everted tonsils are the result of high
negative pressure. The effect of BOAS on gastrointestinal tract is also not negligible. Materials and Methods: A total of 22 brachycephalic dogs which underwent CT imaging of the skull in the time between March 2013 and August 2014
at our Clinic were included in this study. The most common breed was the French bulldog (n 6), followed by pug (n 4), boxer
(n 3), English bulldog (n 2), chihuahua (n 2), Boston terrier (n 1), bullmastiff (n 1), Yorkshire terrier (n 1), Cavalier King Charles
spaniel (n 1) and griffon (n 1).
A total of 31 dogs from different breeds were included in the group of normocephalic dogs. They underwent the CT imaging
of the skull because of different reasons than respiratory disorders.
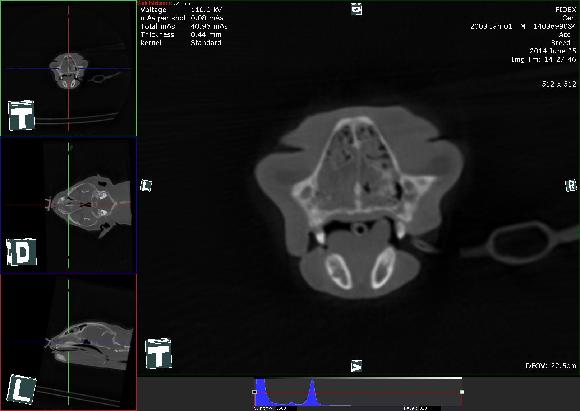
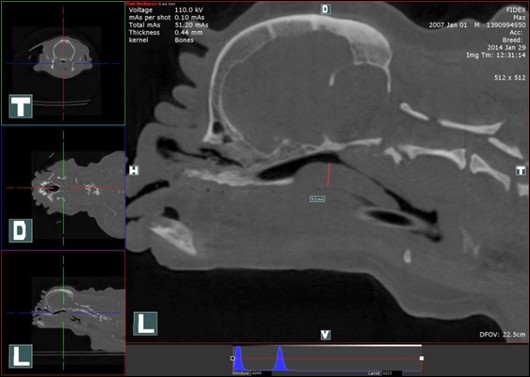
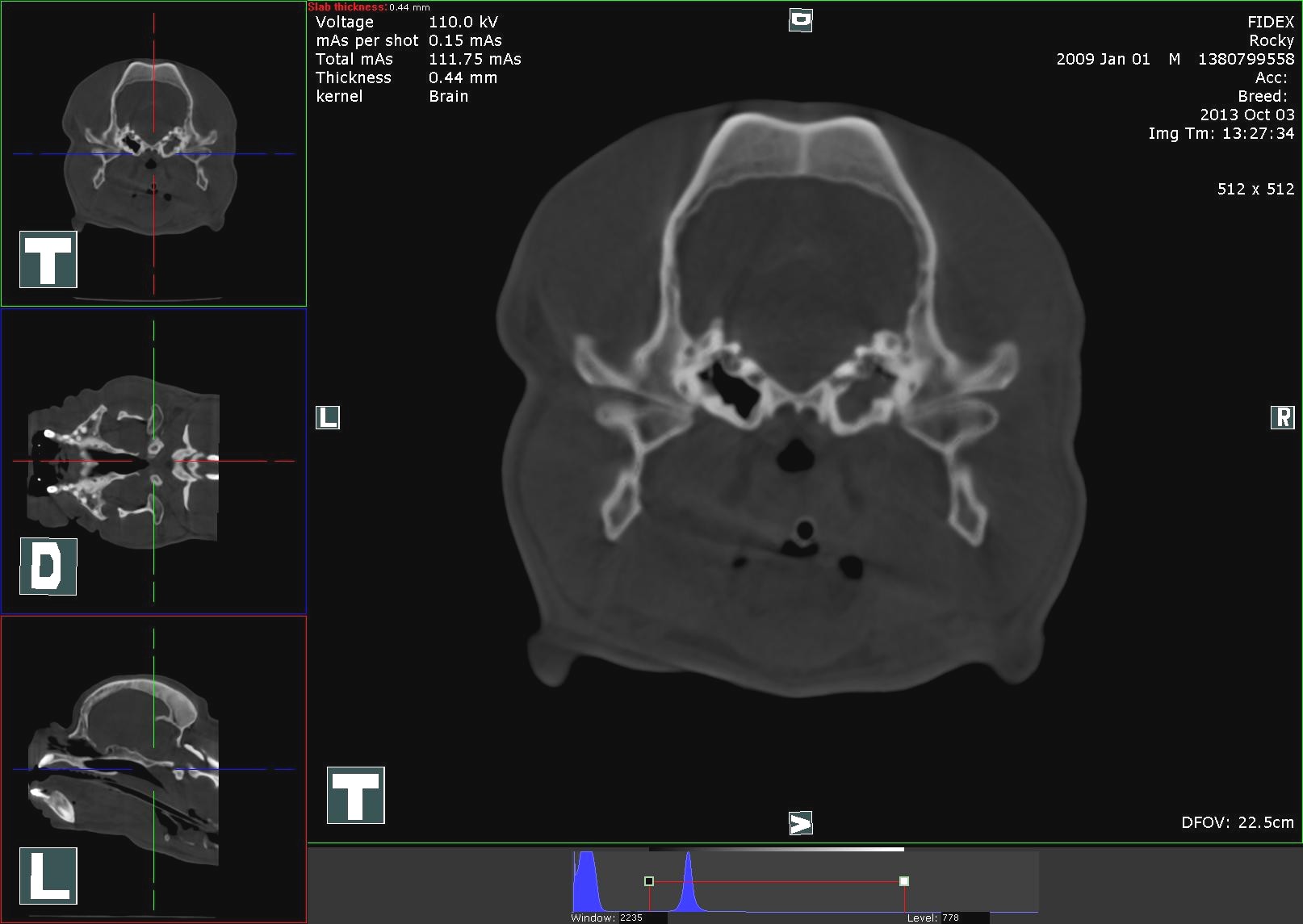
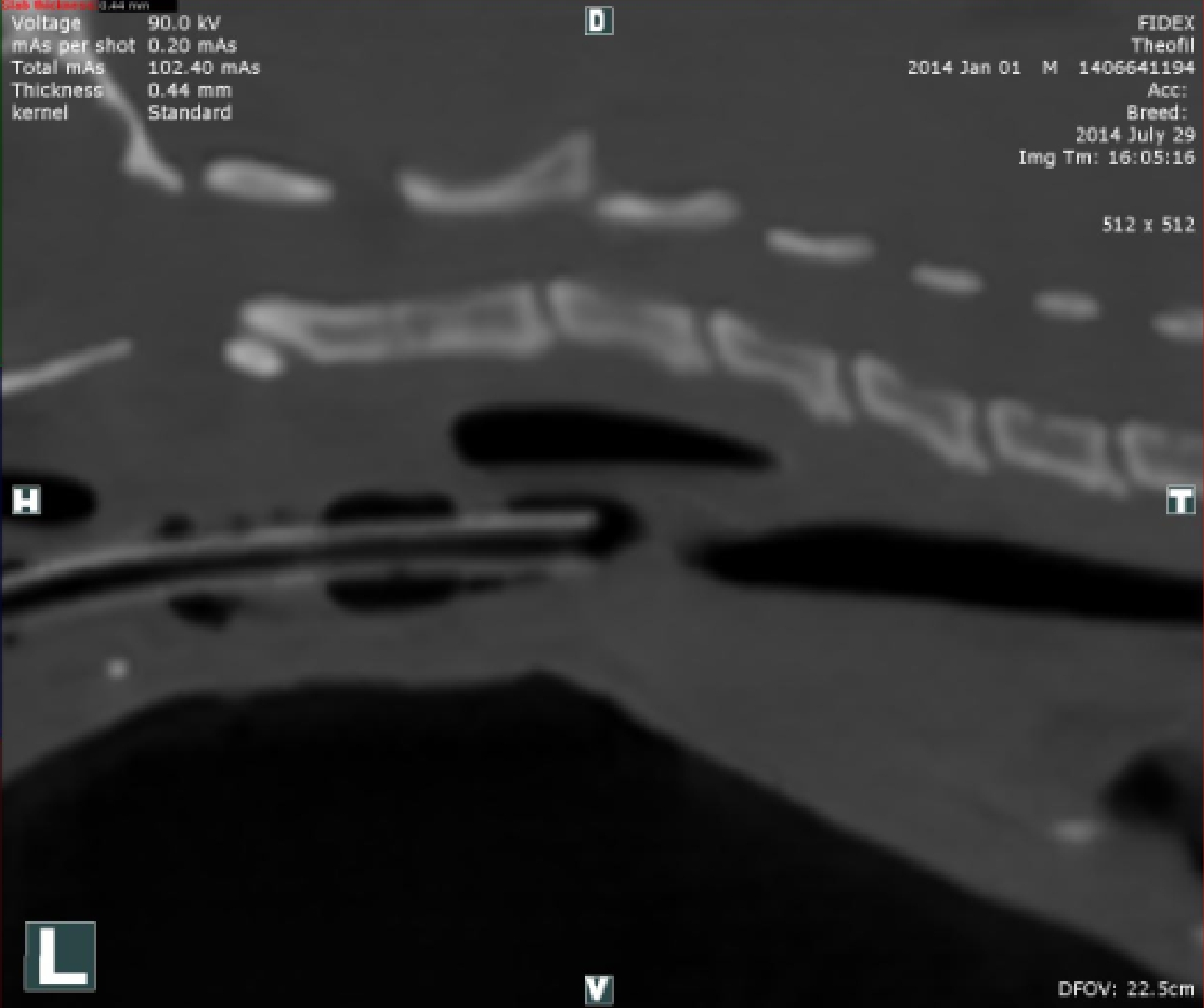
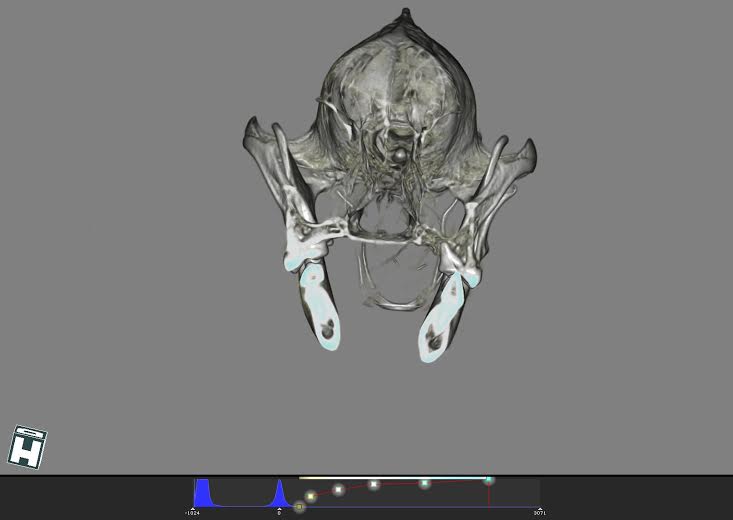
Computed tomographic imaging by Cone Beam CT (CBCT) was used (Fig.2). It is quite a new imaging technology which has
found its use in veterinary medicine in last three years. In contrast with fan-beam CT, CBCT reaches the image by rotation of
one X-ray tube around the patient. Beams passing through the object are caught by dynamic flat-panel detector on the opposite
side and the data is processed for picture reconstruction by the computer. As in a conventional CT transversal, sagital and dorsal reconstruction
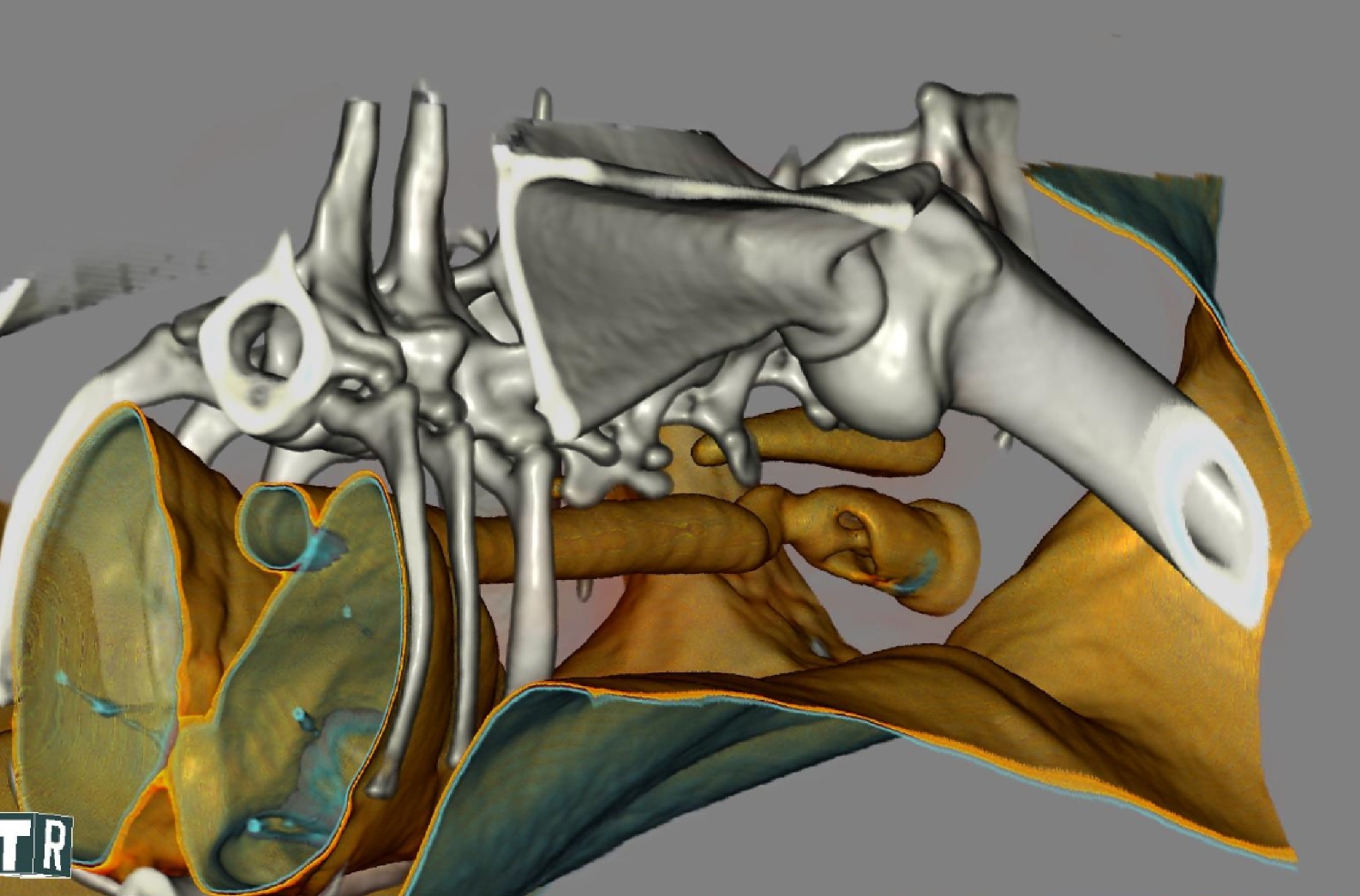
of the image are created. In addition, images can be processed into a 3D reconstruction.
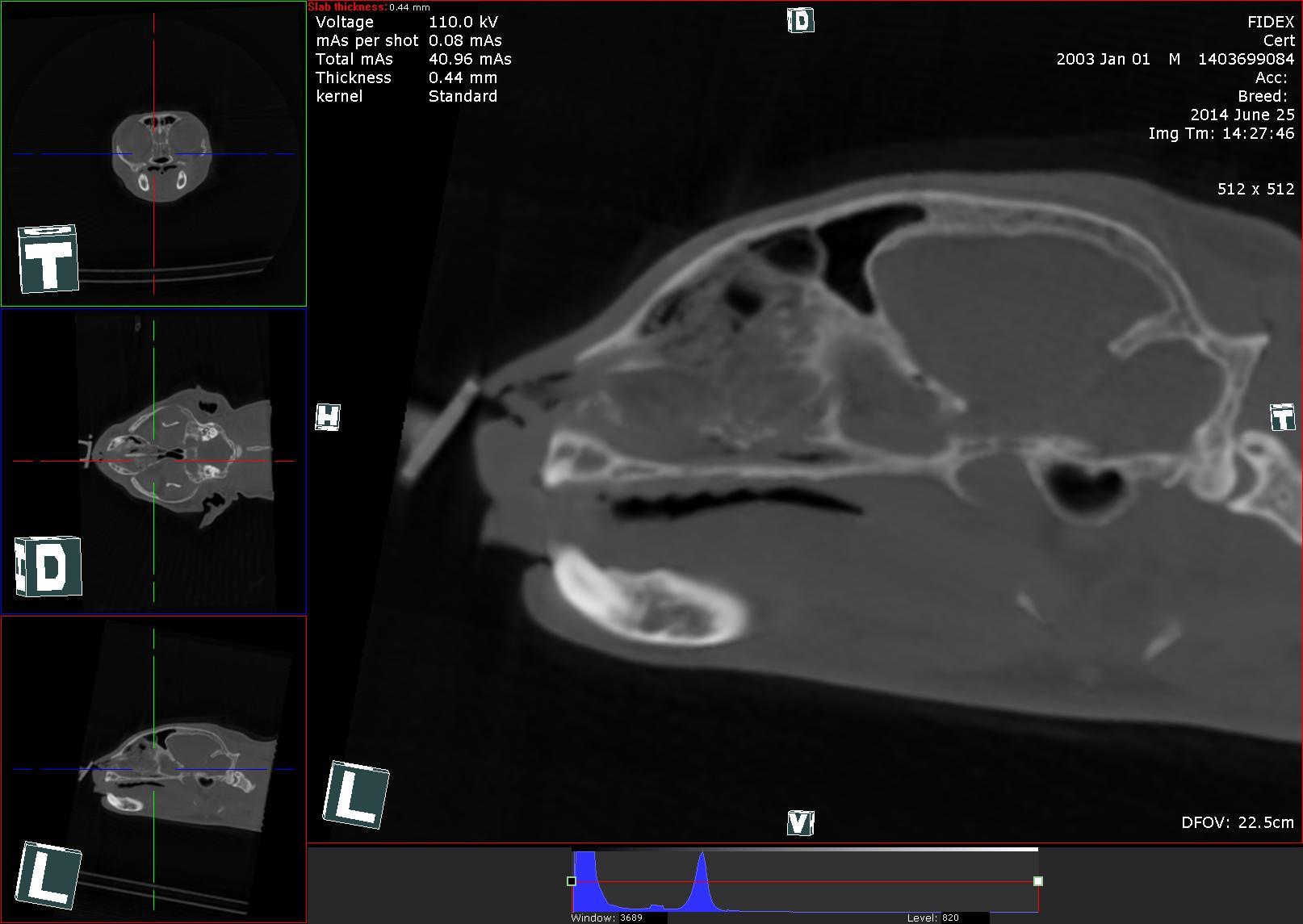
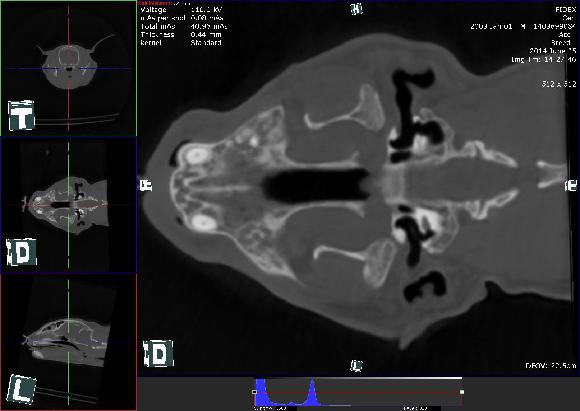
The CT scan was performed on all dogs in sternal recumbency in an extended neutral position under general inhalation anaesthesia with
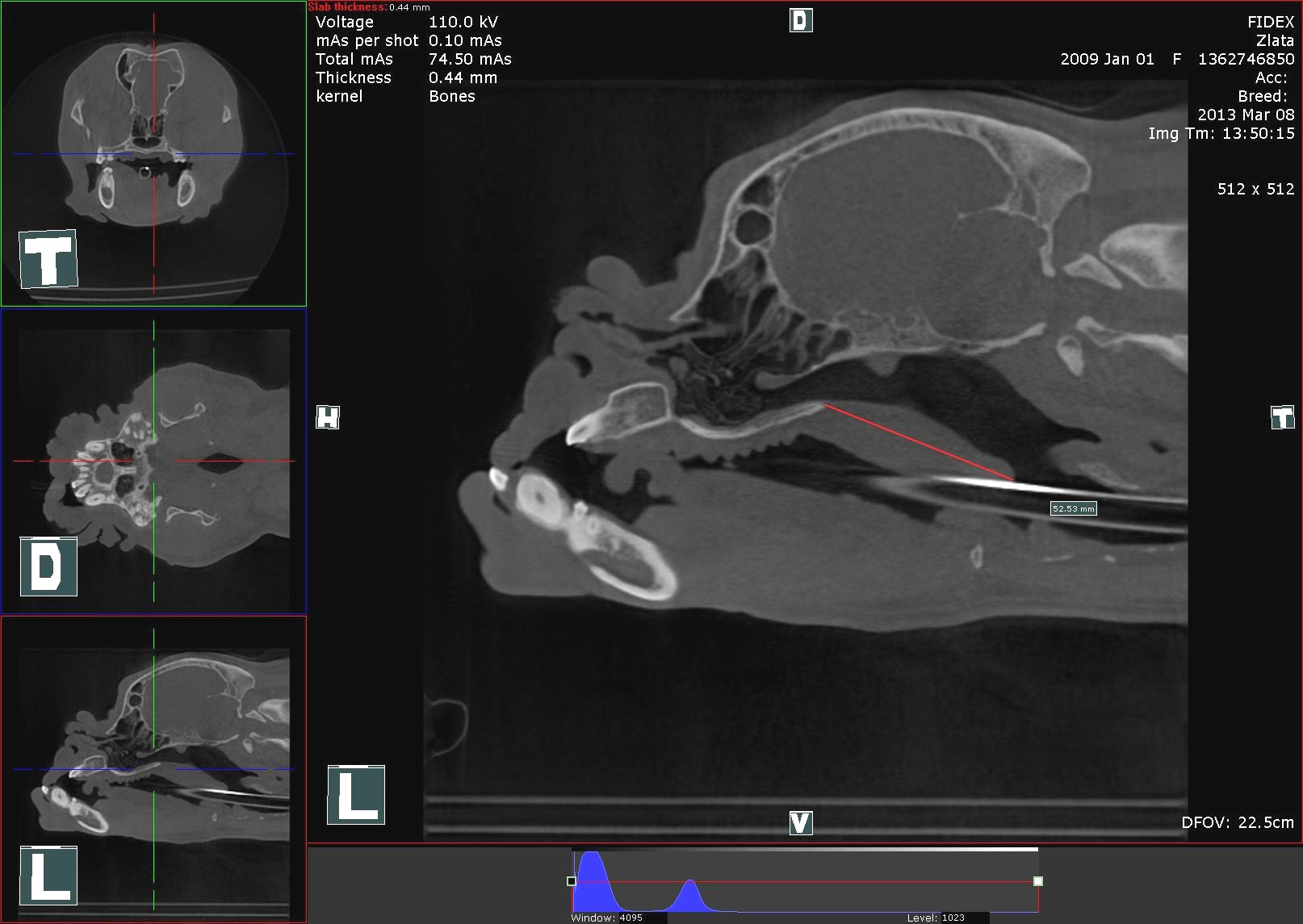
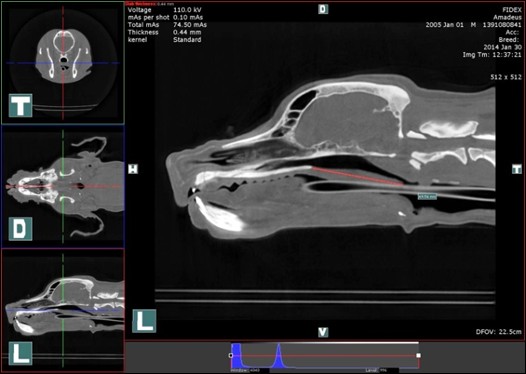
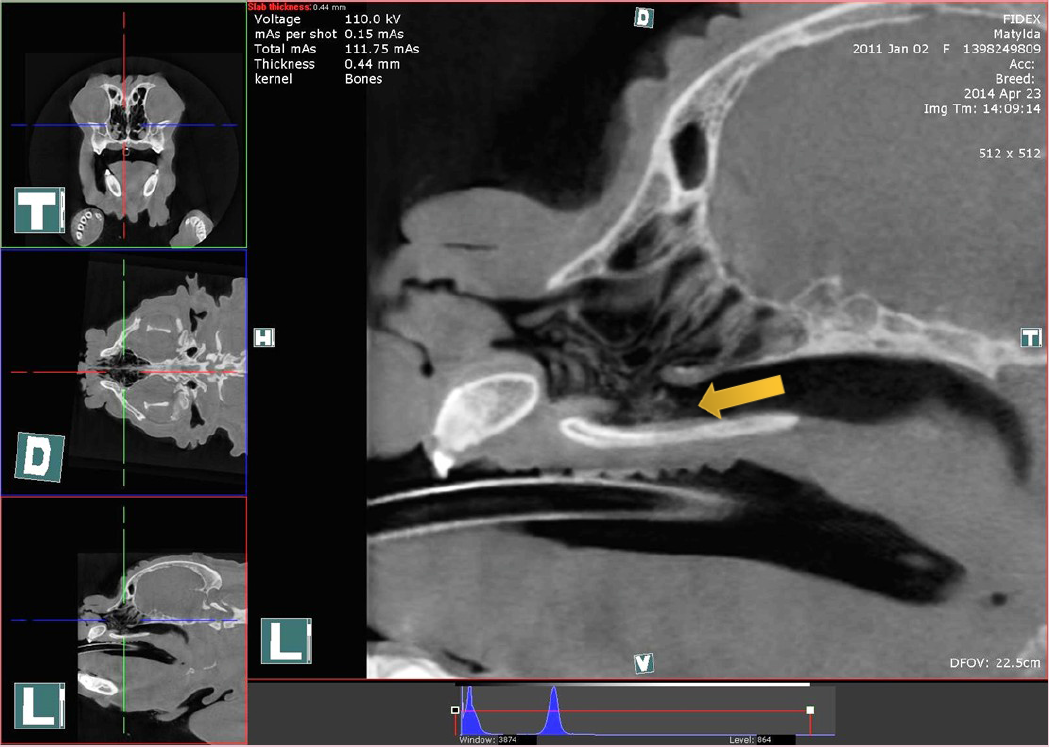
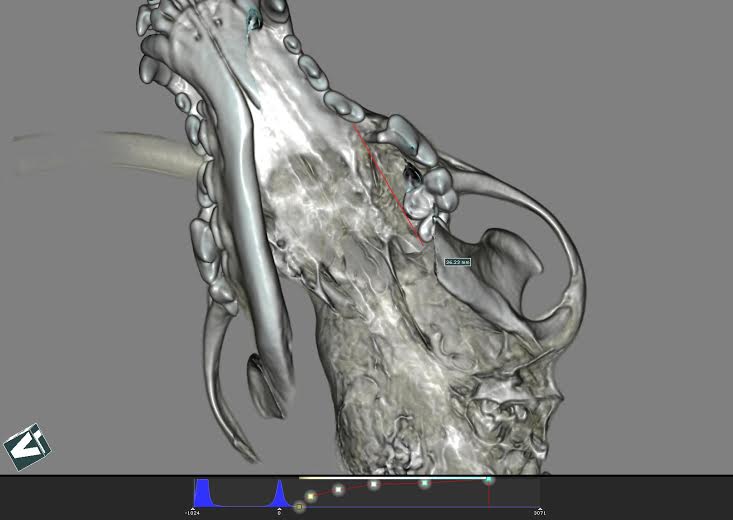
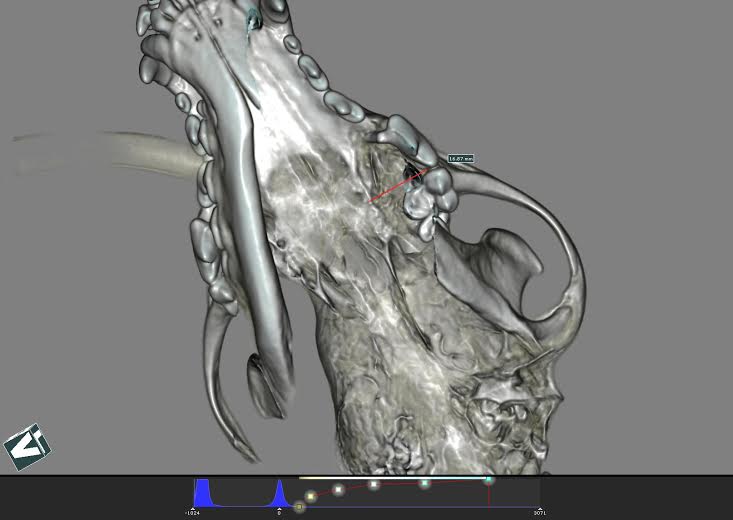
isoflurane in oxygen administered via a cuffed endotracheal tube. The measurements were taken in the midsagittal images at the
level of the deepest point of sella turcica. At this projection the length of the soft palate (SPL) from the caudal margin of the
hard palate to the tip of the soft palate (Fig.3) and the width of the soft palate (SPW) at the level of sella turcica (Fig.4) and the
dorsoventral cross-sectional diameter of the meatus nasopharyngeus (MNP) (Fig.5) were measured. The absolute numbers
could not be compared directly because of the difference in the breeds present. Therefore the ratio between SP length and MNP
diameter and the ratio between SP width and MNP diameter were used. These were summarised as the mean (resp. median)
and were compared between the brachycephalic and normocephalic groups. All the brachycephalic dogs also underwent a retrograde endoscopical
examination of nasopharynx and laryngo-, tracheo- and bronchoscopy for further BOAS evaluation.
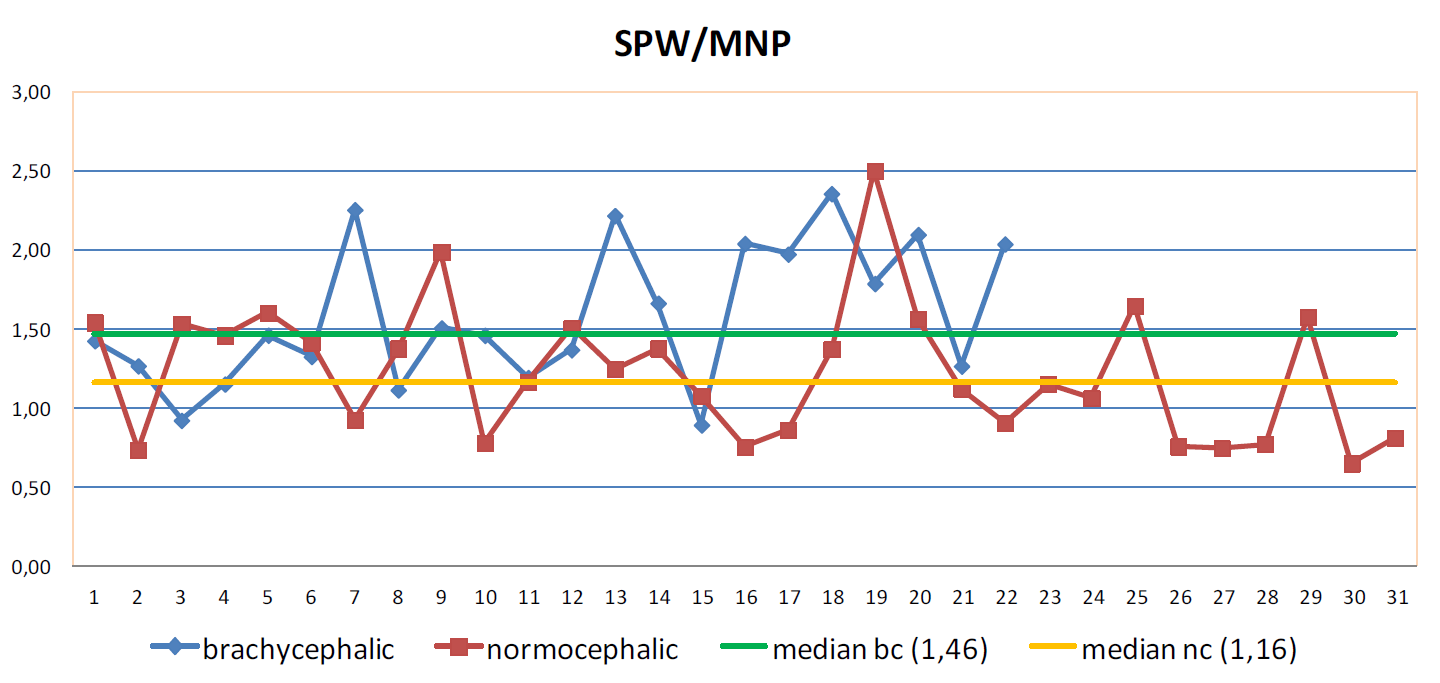
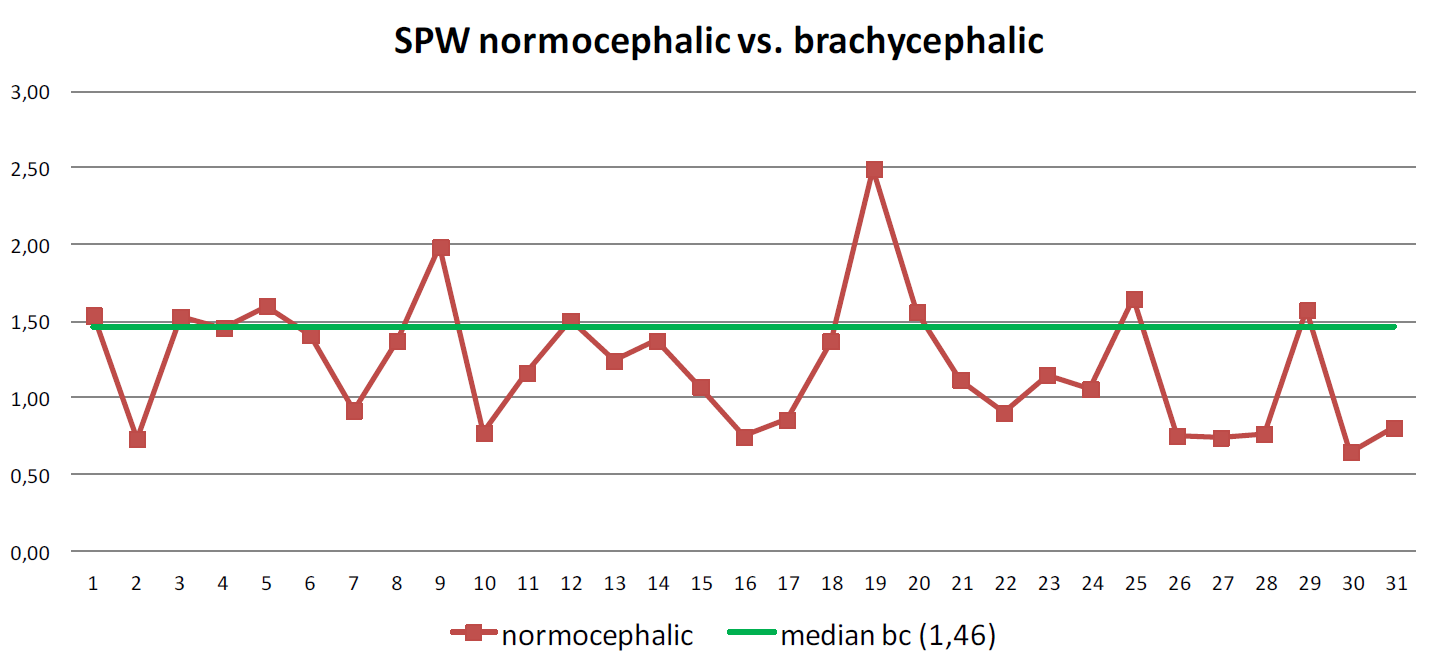
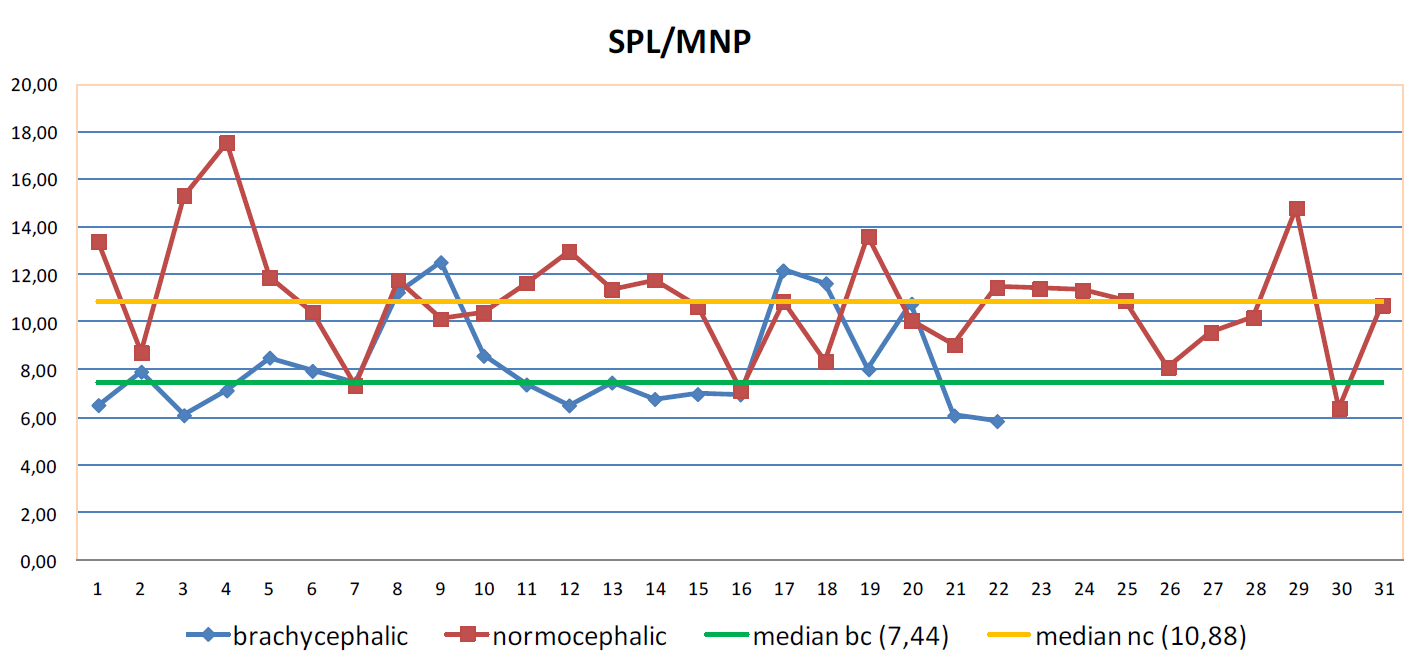
Results: The most obvious finding in our study is that brachycephalic dogs have significantly thicker soft palates compared to normocephalic dogs. (Tab.1) The majority of the normocephalic dogs have the SPW/MNP ratio under the median value of the brachycephalic dogs. (Tab.2)
Discussion: Our measurements confirm the findings in recent studies in which the soft palate width seems to be a very important component in patients with severe signs of BOAS (Brachycephalic Obstructive Airway Syndrom). Whether this thickening is a primary abnormality or a secondary event could not be determined. This thickening could be explained by a muscular hypertrophy, mucosal oedema, or both. This modifications could be induced as an adaptation to the increased intranasal airflow resistance at the level of nares, vestibulum nasi and cavum nasi. Critical attitude has to be taken in assessment of the soft palate length because the measurements were made on static CT scan images on sleeping dogs with endotracheal tube so the dynamic features in awake and asleep states with regard to the respiratory phase could not be compared. Conclusion: Currently, the combination of CT imaging and endoscopy is considered to be a gold standard in evaluation of the severity of BOAS. The endoscopy allows to assess the in situ conditions and evaluate the dynamic airway features during the respiratory cycle. By the retrograde endoscopy the nasopharynx diameter, mucosal and/or lymphatic tissue hyperplasia, caudal aberrant turbinates presence can be detected. (Fig.7) The trachea and bronchi are then observed for the presence of collapse or other anomalies. Interestingly, the left-side cranial subsegmental branches are affected more often than the right-side bronchi.4 Also, it has been recommended by some authors to assess the GI tract during the endoscopy because of the presence of typical gastrointestinal disorders in these breeds. Some evidence-based studies show better recovery from corrective surgery of BOAS in patients treated simultaneously with antacids and prokinetics. Computer tomography is a non-invasive imaging method that permits a detailed assessment of the entire upper airways. Especially, the nose structure of brachycephalic dogs is very complicated. Oechtering and others utilized this in 2007 and they proved the hypothesis of abnormal intranasal structures such as rostral and caudal aberrant turbinates, narrowed asymmetric and distorted nasal passages, mucosal folds, deviation of the nasal septum, nasal conchae occupying the nasal passages and meatus nasopharyngeus etc. (Fig.8) This clarified why the outcome after the surgical correction of stenotic nares, elongated soft palate and everted laryngeal saccules is not always satisfactory. Using the CT imaging also allows us to asses the structural characteristics of the pharynx, especially the length and width of the soft palate.
References:
Case of the Month July 2014: Female Domestic Short Haired Cat Severe Chronic Inspiratory Dyspnoea Jan Hnizdo Animal Clinic, Prague http://www.animalclinic.cz History: 11-month old female domestic short haired cat, 2kg, was referred for severe chronic inspiratory dyspnoea. The cat had been found as a 3month old kitten. Already at that time the kitten showed some signs of inspiratory distress. During the last weeks the symptoms progressed further. At time of presentation the patient showed very severe inspiratory distress with paradoxical movement of the sternum. During manipulation the cat become cyanotic and had repeated hypoxic syncopes with cramping. Clinical exam: Subcyanotic mucus membranes, exercise intolerance with syncopes. Tachypnoea with severe inspiratory labour. During inspiration a marked flatting of the thorax and paradoxical movement of the sternum appeared. Nostrils were clear. The patient was stabilised with tranquilisers in an oxygen box for a few hours before anestesia. Xray exam: Thorax LL and DV were normal. Endoscopy: There was some mucus accumulation in the larynx. Caudal to the larynx appeared a marked narrowing and tracheal stenosis with a mucosal poach bulging in to the lumen of the trachea. The stenosis allowed the endoscope to be passed easily further caudally. The rest of the trachea and bronchi appeared normal. (fig. 1 and 2).
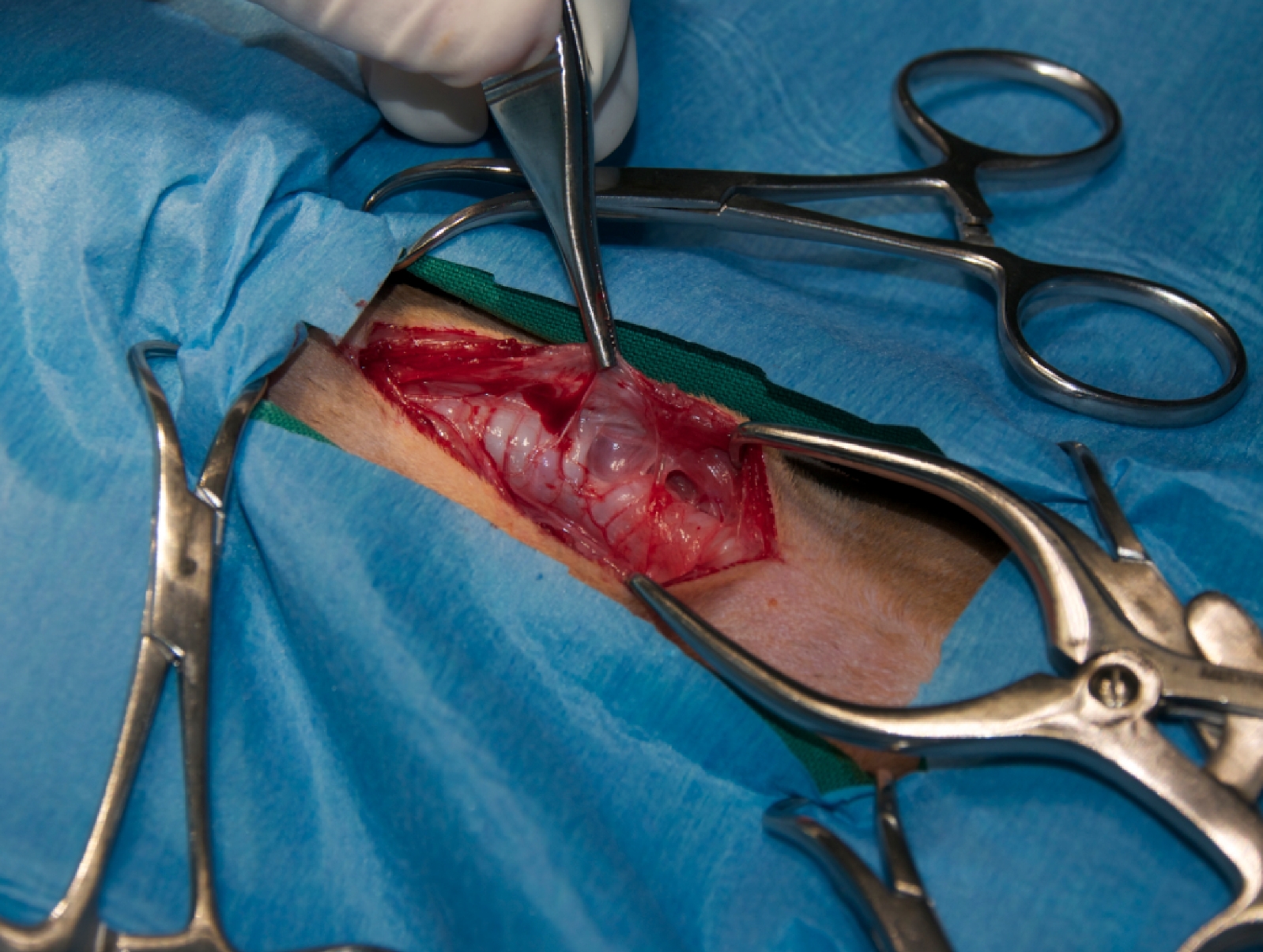
CB CT exam: Following the endoscopic exam the cat was re-intubated (only to the level of the larynx) and connected to an open circuit with mechanical positive and pressure ventilation. The cat was positioned in dorsal recumbency with the head away from the gantry. Native scan showed a marked irregular tracheal narrowing of about 15mm caudal to the larynx. The tracheal rings were open (missing) on a segment of about 18mm dorsolaterally from the right site. The trachea was crooked and the lumen was at the narrowest part only about 2mm (versus normal diameter of 6.5mm). The rest of trachea and bronchi was considerd normal.
Therapy: Based on the CT findings (segmental aplasia of tracheal rings with severe narrowing and stenosis), surgery was recommended as tracheal stenting did not promise much success. Following the CT findings the damaged segment of the trachea (about 20mm) was resected en block. End to end anastomosis was performed routinely with single interrupted sutures through the tracheal rings, with some circumferential release sutures (fig 6, 7). Comment: Inherited segmental hypoplasia of tracheal rings is considered an extermely rare event, there are no case reports in cats published yet.
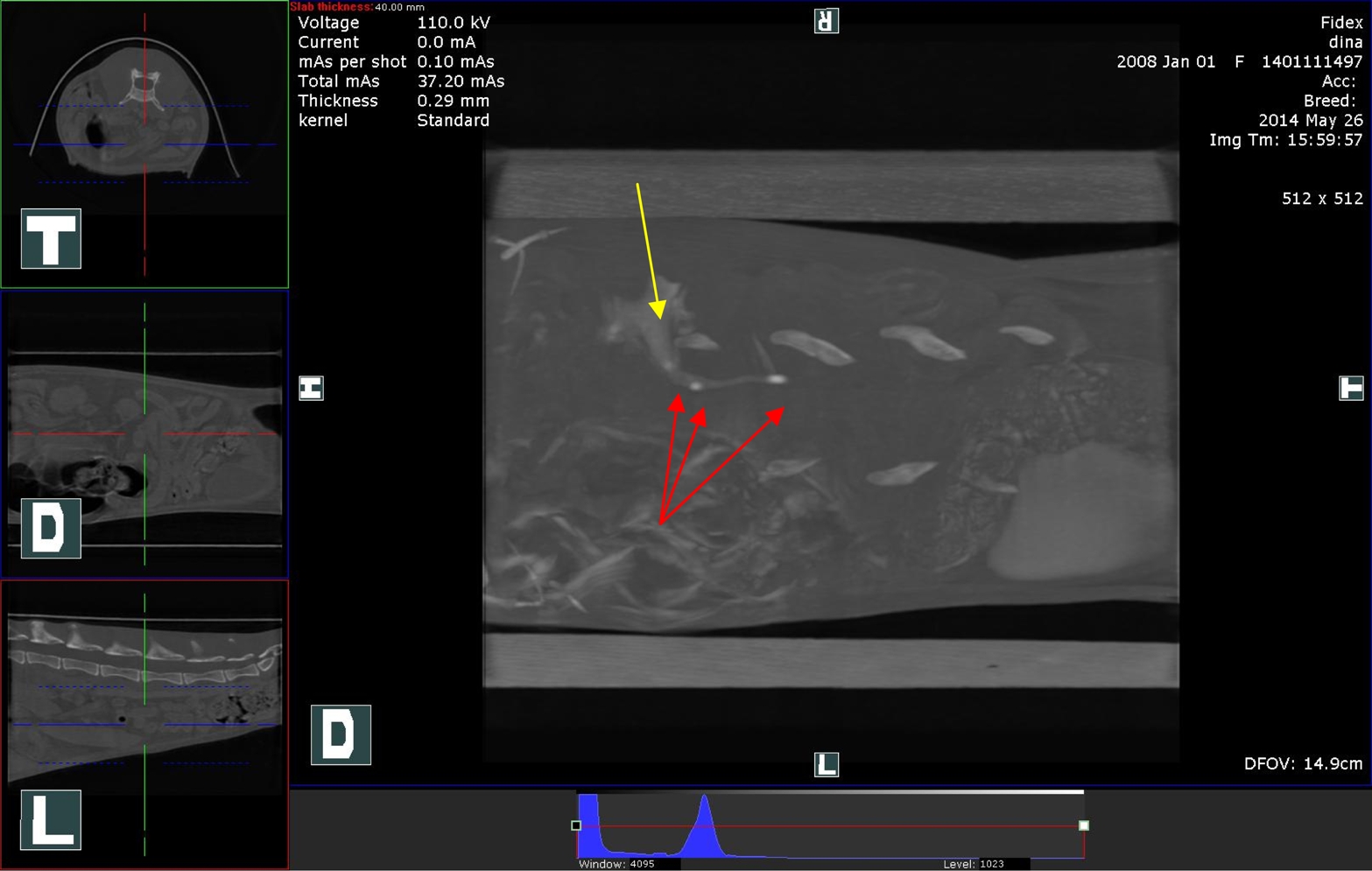
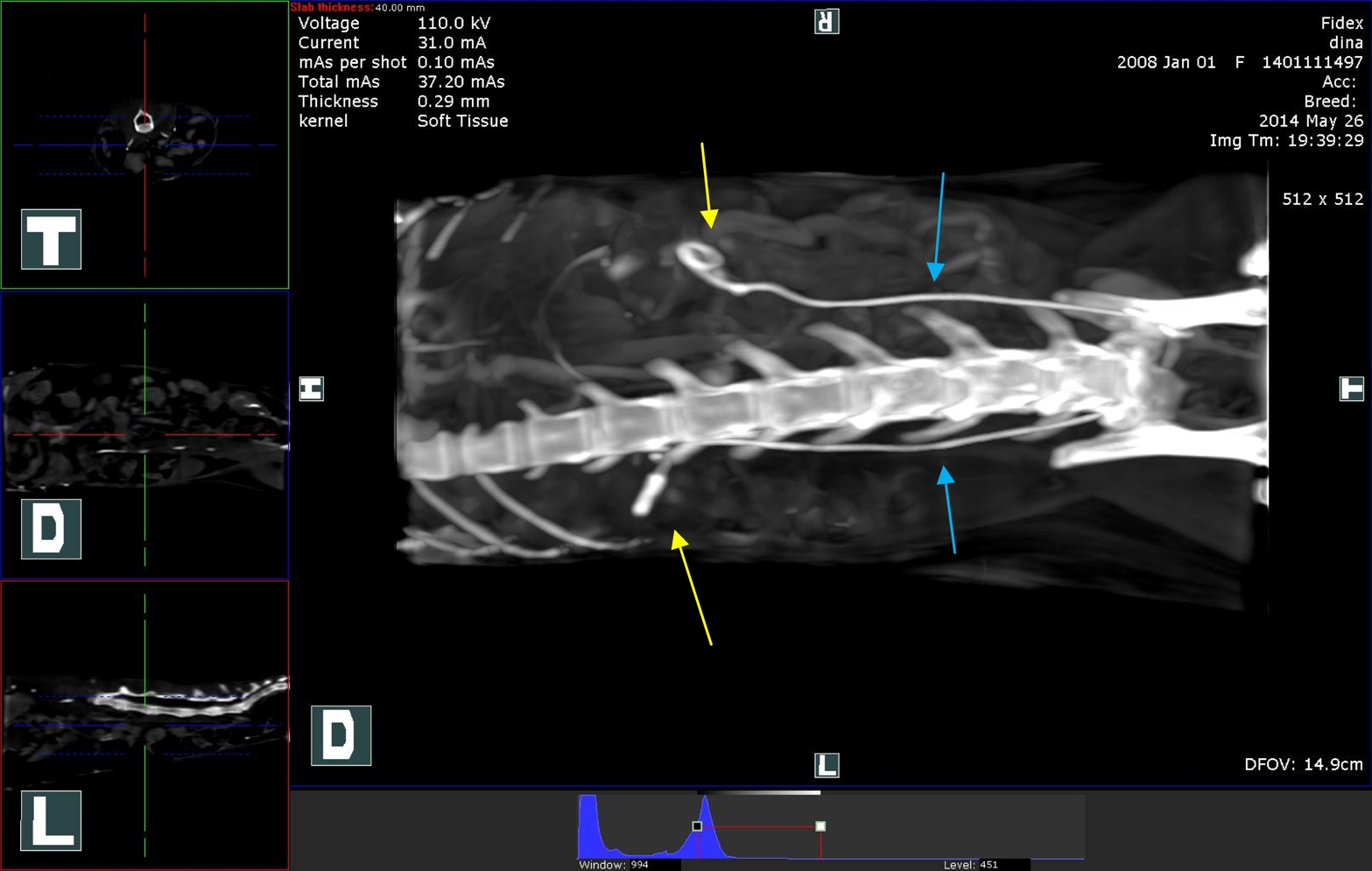
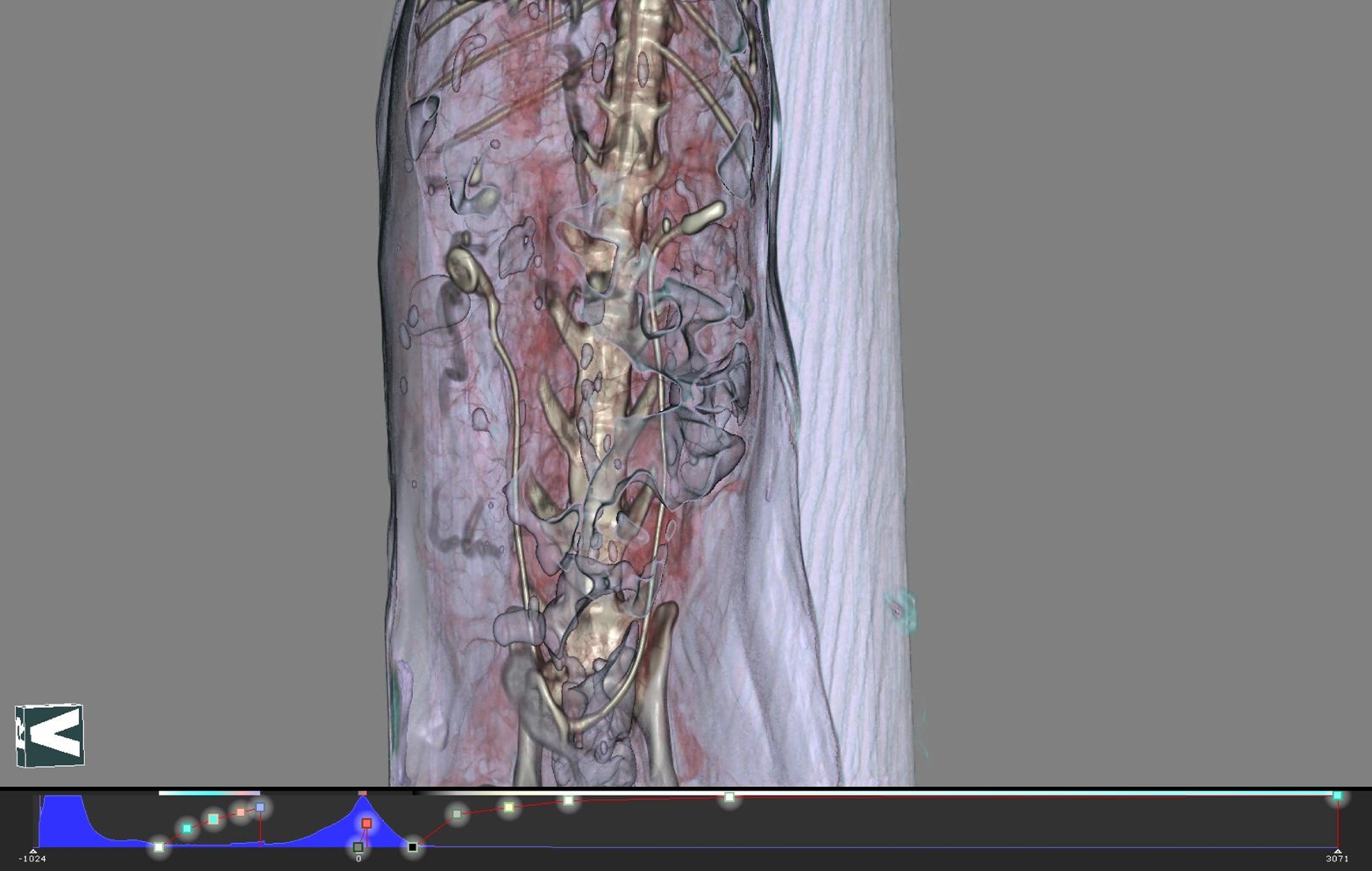
Case of the Month July 2014: Ureteral Calculi in a Persian Cat Dr. Bertrand Vedrine, Clinique veterinaire de Boos - France History: Anorexia, lost of bodyweight, apathy since 1 week. Blood sample reveals an acute renal failure (uremia = 3.63 g/L, creatininemia = 185 mg/L, phosphoremia = 188 mg/L) and ultrasonography the presence of ureteral calculi. Medical treatment: Medical therapy was tried during 5 days with no resolution of the acute renal failure and limited quantity of miction. The 5th day uremia = 2.3 g/L and creatininemia = 91.4 mg/L. An ureteral stenting procedure was decided Pre-operative CT: An uroscan was performed before surgery:
Surgery: Ureteral stenting (2 F, Infiniti Medical) was performed on each side. On the right side, an ureterotomy was needed to remove the biggest calculous before stenting. On the left side, a stenosis of the ureter was present and the placement of the stent was very difficult even with the use of a dilatators. Post operative DR and CT: An uroscan was performed postoperatively. The stents were placed in right way between each kidney and the vesical bladder. Permeability of the left ureter was restored by the stent. Post-operative: The cat died rapidly because of the lack of improvement of the acute renal failure.
Case of the Month June 2014: Oral Sarcoma History: patient reffered with histopathologically confirmed oral sarcoma for further diagnostics and surgical management. Partial surgical removement was already provided. Clinical Examination: ulcerative superficial lesion on a left dorsolateral part of the hard palate was seen. Submandibular and prescapular lymphonodes were without enlargement. Other organ systems seemed to be wihout any clinical findings. Cytological findings: normal lymphocyte population, small amount of morphologically normal lymphoblasts (5-15%) and small amount of plasmatic cells was detected in all examined samples. Contrast head CT findings: osteolytic maxillar mass with a high contrast enhancement surrounding 207-210 was found, other visible structures were without detectable changes Contrast chest CT (using an i.v. contrast and breath holding system): Surgical management: Bucal incision for a better approach to the affected area was provided. The tumor was removed by caudal maxillectomy (207-210 incl. part of arcus zygomaticus). About 50% of the hard palate was removed and the defect was covered by a wide mucosal flap adapted to the rest of the hard palate mucosa. Histopathological Findings: Malignant spindle cell tumor was found with a suspicion of peripheral nerve sheath origin.The neoplasm did not reach the sample margins in all examined sections. Further therapy: After the wound was completely healed, the patient was reffered for radiotherapy (VetMedUni Wienna). Comment: Histological examination revealed a malignant mesenchymal neoplasm. Possible origin is in a particular Schwann cells of the peripheral nerve sheath. This type of neoplasm has a tendency for recurrence due to infiltration along the nerve fibres. The metastatic potential is usually low. Surgical removement with a wide margine combined with radiotherapy seems to be the best therapeutic option in cases like this.
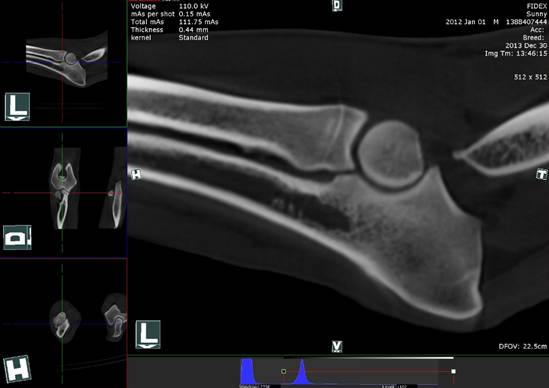
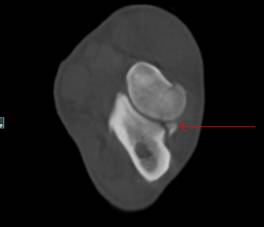
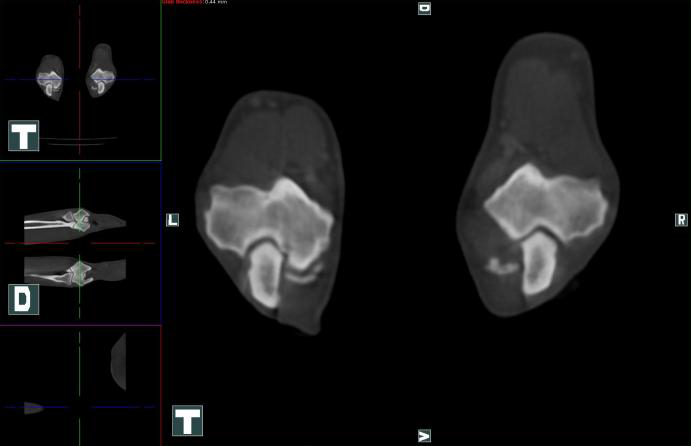
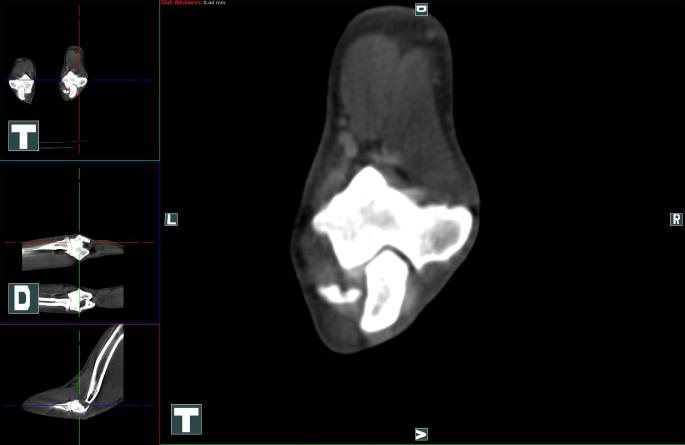
Case of The Month : Orthopedics Mastiff with frature/fragmentation of the lateral coronoid process J. Hnizdo Animal Clinic www.animalclinic.cz History: Tibetan mastiff, male, 2years old, 55kg, was presented for acute onset of lameness of the right front limb. There was no clear history of trauma but the dog had escaped for a few days in the forest and had come back home lame. Physical exam: general health check was unremarkable. The dog was lame on the right front limb, constant, mixed lamenes grade II/VI. There was some painfull reaction at maximal flexion of the elbow joint, othervice the exam was unremarkable. Radiology: no abnormal findings were noted on Xrays in two orthogonal views of the elbow joint (fig. 1). CB CT: the dog was anesthesized and positioned in ventral recumbency, facing towards the gantry with both front limbs extended and head flexed away from the gantry. The dog was taped firmly in position. Throughout the scan it was ventilated with an intermittent breath holding system (PEEP, frequency setting 10 breaths/min, two breaths between the scanning cycles). CT setting: Voltage 110kV, 0.15mAs/shot, thickness 0.44mm. Bone reconstruction mode was used. Both elbows were considerd congruent on the sagittal and dorsal projection, not exhibiting any signs of degenerative changes (fig 2). Both medial coronoid processes were intact and without signs of fragmentation or subchondral fissures. On the transversal view there was a clear separation of the lateral coronoid process (fig. 3 and 4). On top of that, a thin partial fissure was visible in craniomedial to caudolateral direction through the radial head (fig. 5, 6). No other changes were noticed on the CT scan. Diagnosis: frature/fragmentation of the lateral coronoid process, fissure of the radial head. Arthroscopy was performed through the standard medial port. The fragment of the lateral coronoid process could be clearly visualised, but it was impossible to reach the fragment through the medial portal site (fig 7). Technically it was not possible to establish a third port from the caudolateral site. The fissure of the radial head was largely subchondral and only hardly visible on arthroscopy. No attempts were made to fix the fissure. Due to the technical difficulties of reaching the fragment through the arthroscopic portal, a caudolateral miniarthrotomy was performed and the fragment was removed in toto. The joint was flushed and sutured routinely. Outcome: the dog was lame-free ten days post operative. It shows no clinical problems until now (5 months post operative). However, some progression of osteoarthosis is expected in the long term. Comment: the presented case is to our knowledge the first documented case report of an fragmented lateral coronoid process in a non displastic dog. The ethiology is unclear but trauma is suspected in this case. In dogs with elbow dysplasia and especially with progressive secondary degenerative joint disease, lesions of the lateral coronoid process may be recognized during arthroscopy more often. CT exam was in our case the only diagnostic modality that could confirm the correct diagnosis preoperatively as other radiographic findings were completely absent. Removing the fragment seems to lead to complete recovery in this case.
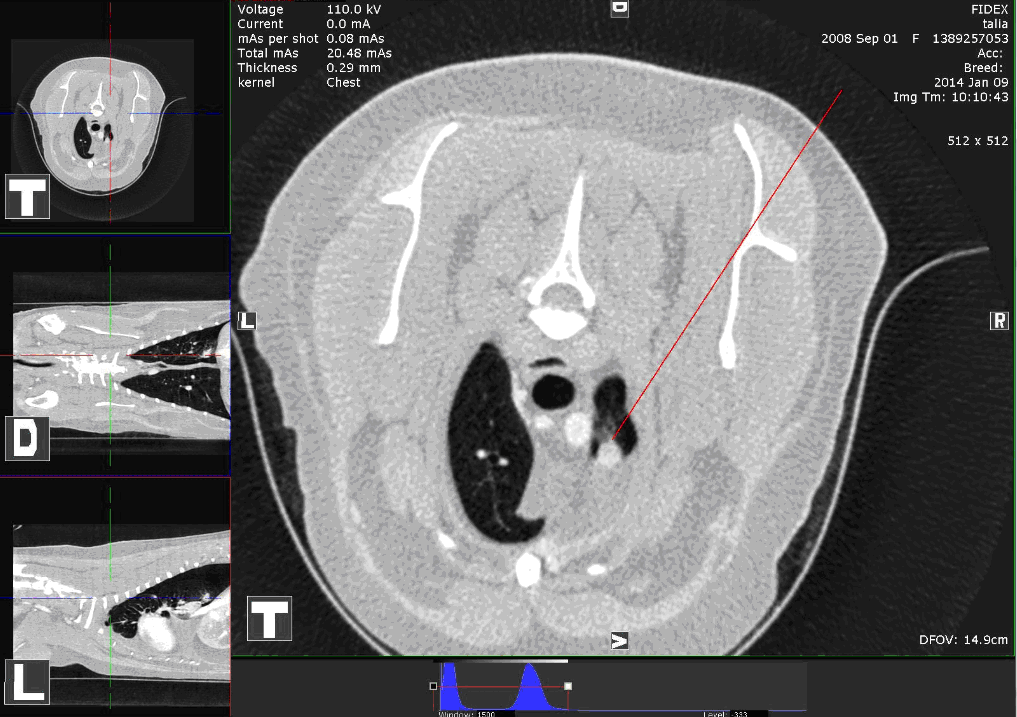
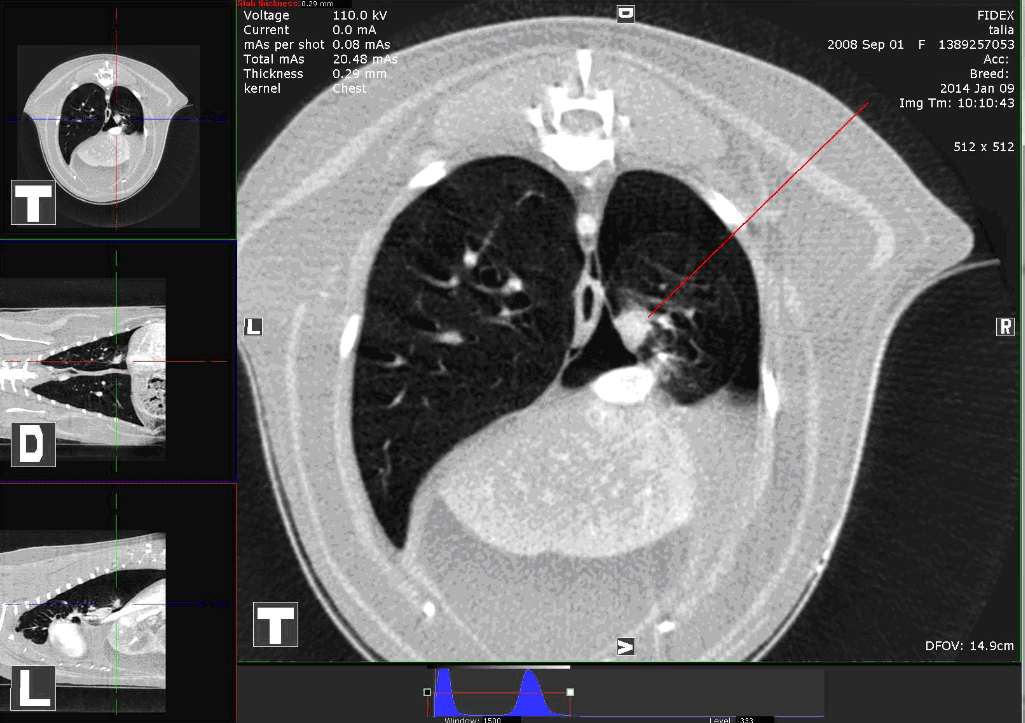
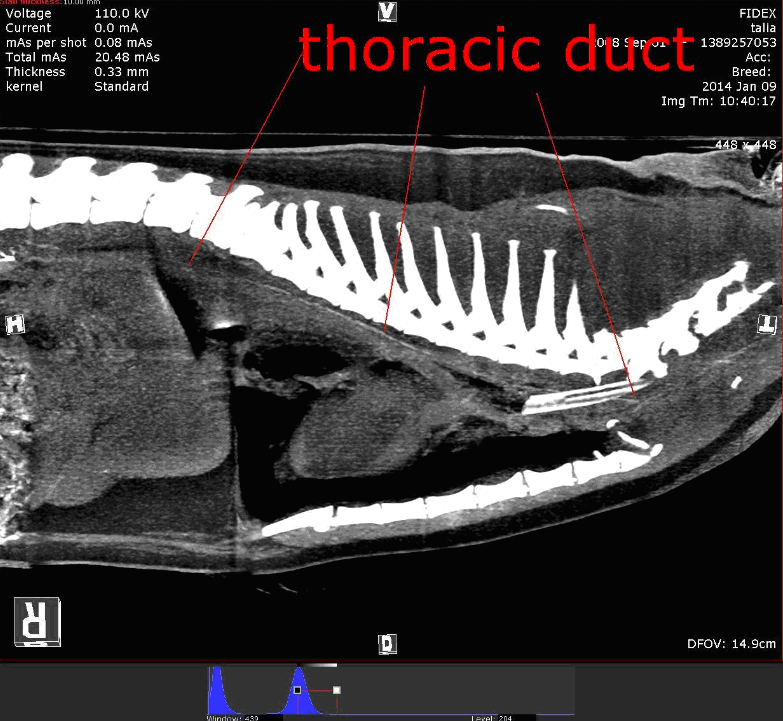
Case of The Month : Chylothorax This case has been submitted by Dr Roland Rigori of Bourgoin Jallieu in France. Patient: Cat, DSH, female spayed, age: 5 years Case history and Physical examination: The patient was with a dyspnea and cyanotic aspect. An x-ray examination showed substantial thoracic effusion. A thoracic puncture without anesthesia withdrawal 200ml milky liquid with many cells on a slide. Test 50-50 with ether shows a clarification of the effusion . Chylothorax was supected. The Cytologist confirmed this diagnosis. After few days with medicinal treatment, the cat was referred to our Clinic. An ultrasound heart exam show a pericardic effusion (with tamponade). A tab in order to remove most of the liquid was done. Then a CT scan was performed to:
3 CT scans were performed. 3. CT after 3 ml injection of iodine (300mg/ml) in a mesenteric Lymph node (for the thoracic duct). Findings: The CT shows bilateral chylothorax associated with many pulmonary nodules and contrast uptake in multifocal pleural plaques. Diffuse pulmonary granulomatous bronchopneumonia (parasitic ? cryptococcus? eosinophilic?) The origin of Chylothorax is unclear from the images but potentially connected to the pulmonary changes. A fecal flotation test and a tracheal + pulmonary wash was done. The flotation show nothing but the pulmonary wash shows inflammatory changes (inflammation cells, no bacteria). Conclusion. It was decided to forego immediate surgery but use a medical treatment (amoxicilline-dexamethazone-fenbendazole). One month later, the cat is OK without any further tabs necessary.
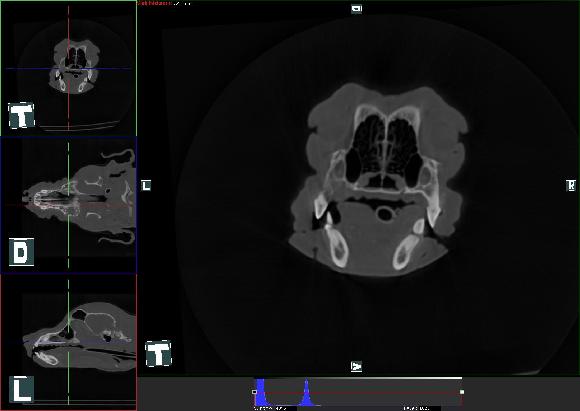
Case of the Month March 2014, submitted by History: 5 years old female Dachshund presented with unilateral nasal discharge and prominent soft tissue swelling on the dorsal aspect of the nose. According to the owner, she had problems with unilateral [left sided] discharge since age of 3 years. A month ago, biopsy was taken and rhinoscopy of the nose was done by another veterinarian. The final diagnosis was rhinitis and patient was treated with enrofloxacine. However, only mild improvement was observed. Physical examination: Patient was bright, alert, had a normal temperature of 38.9C. Severe nasal stridor and left sided epistaxis was noted. The remainder of physical examination was normal. CT images Tranverse CT image reveals a soft tissue density mass occupying left and most of the right nasal cavity with lysis of the dorsal left nasal bone.
Findings: There is a large soft tissue mass occupying most of the left and right nasal cavities from the level of the incisors to the cribriform plate. The turbinates are absent from the rostral and mid nasal cavity in the area occupied by the mass. The turbinates are present within the soft tissue mass in the caudal nasal cavity. This mass causes extensive multifocal lysis of the overlying maxilla and the mass extends dorsally through the defects in the maxillary bone. The maxillary bone along the medial left orbit is lytic but no extension into the retro-orbital space is noted. The cribriform plate is intact. Soft tissue material is present in both frontal sinuses and the left sphenoidal recess. One of the left mandibular lymph nodes is enlarged compare to the ones on the right. The left medial retropharyngeal lymph node is also enlarged. Conclusions: Primary nasal neoplasia with extensive maxillary bone destruction. Likely left mandibular and medial retropharyngeal metastatic lymphadenopathy. Final diagnosis: Nasal adenocarcinoma with extensive bone destruction and metastatic lymphadenopathy. Treatment: The only option in this case is radiation therapy. Treatment was denied due to financial reasons. Prognosis in this case without recommended therapy is poor.
Dr. Richard Kilburn, DVM of Countyline Animal Hospital in Naperville, IL History: 11 year old cockapoo, mildly overweight. Subtle lameness of left front leg, unresponsive to Rimadyl. 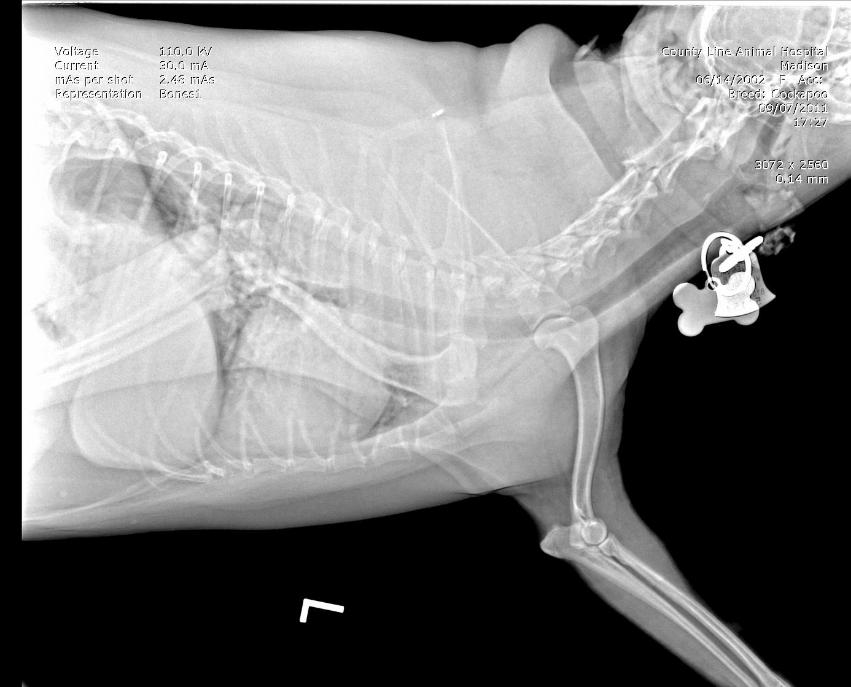 Figure 1: X-Ray of upper left leg and spine Findings from Fig. 1: The lateral xray of the upper leg and spine reveals a very distorted looking (cervicle vertebra C-7). Conventional interpretation would be a vertebral body being destroyed [typically tumors cause this, which would be a death sentence for the dog].  Figure 2: CT Findings from Fig. 2: CT was performed. My interpretation was that the cervicle vertebra and disks were normal. The images were shipped off to a boarded radiologist, who found a tumor (lipoma) behind the dorsal left scapula and speculated the mass effect was causing the lameness. Surgery to remove the benign tumor was scheduled. On the day of the surgery I was ill and I canceled the surgery. One week later, Madison was normal. The surgery was never performed.  Figure 3: Findings from Fig. 3: Later, examining the CT I discovered a faint bulging disk at C-7, T-1. Re-visiting the history and
symptoms, I concluded the real problem was the bulging disk, not the tumor (plus my boarded radiologist failed to
detect this pathology.
Dr. Jan Hnizdo, Animal Clinic , Prague CZ, www.animalclinic.cz Patient: Irish setter, 3.5 years old, female, intact. Anamnesis: intermittent right front limb lamenes since one month. Only short term improvement after NSAIDs. Physical exam: grade II/VI lameness right front limb. Pain on maximal extension of the right elbow joint. Otherwise normal. Radiology: both elbows no signs of elbow dysplasia. Bilateral radiodense bodies caudodistal to medial epicondyle. Otherwise normal (Fig. 1).  Figure 1. Ultrasonography: Hyperechoic structures located inside the flexor muscles distally to their origin. Mild joint effusion. CT scan: Patient in ventral recumbancy, thoracic limbs stretched towars the gantry, head flexed away from the gantry. Inhalation anesthesia with mechanical breath holding. Setting: half beam (d=15cm), 110kV, 0.1mAs, two volumes. Contrast study: iohexol 300 at a dose of 2,5 ml/kg as a fast bollus at the beginning of the scan. Scan lenght 19.5cm, reconstruction algorithm: standard. Both elbows congruent, medial coronoid processes bilaterally without evidence of fragmentation, normal subchondral bone (Fig. 2). 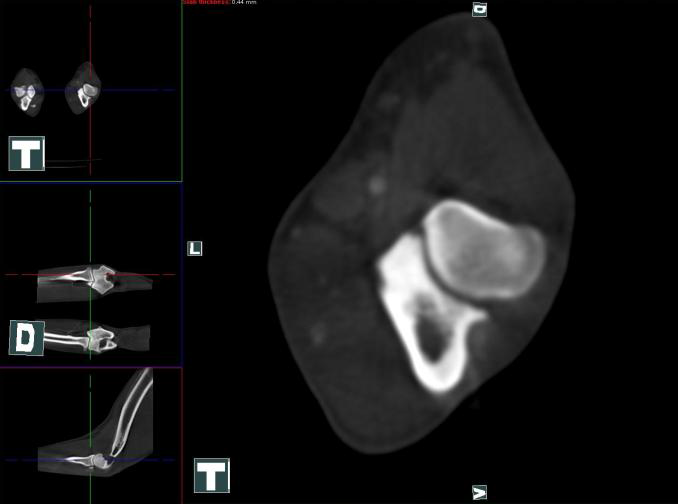 Figure 2. Caudal epicondyles bilaterally irregular, bony spurs (fig. 3, 4) inside the flexor muscles (m. flexor carpi radialis).
Close to the insertion longitudinal bodies of bone density, decent contrast enhancemet at the insertion on the right side (Fig. 5, 6).
What’s your diagnosis? Flexor enthesopathy is a recently recognized syndrome, which can cause significant clinical signs in canine patients. Presently two forms are distinguished: the rare primary enthesopathy as described in this case, and the relatively common concomitant enthesopathy (together with other dysplastic and/or degenerative changes of elbow joints). The ethiology of primary flexor enthesopathy is unclear, but repetitive microtrauma to the intraarticular part of the muscle origin (enthesis) is suspected to be the cause. This is in analogy to medial epicondylitis in people („golfer’s elbow“). The main problem is the differentiation of the two forms. Besides that, similar radiologic changes can appear as a clinically irrelevant, incidental finding in a dysplastic elbow joint. If concomitant flexor enthesopathy is diagnosed, usually the primary cause (e.g. medial coronoid diesease) has to be addressed therapeutically. In the presented case report, the diagnosis of primary flexor enthesopathy was suspected based on radiologic signs and ultrasound findings. The final exlusion of secondary, concomitant enthesopathy was possible only based on the CT findings. During the following arthroscopic exam primary flexor enthesopathy was confirmed (fig 7). Therapy was based on local infiltration with a methylprednisolon acetate.  Figure 7. The correct diagnosis of primary flexor enthesopathy is based on the combination of different diagnostic techniques. Special emphasis must be focused on the differentiation between primary and secondary enthesopathy. For this purpose the author considers CT to be the most usefull diagnostic modality.
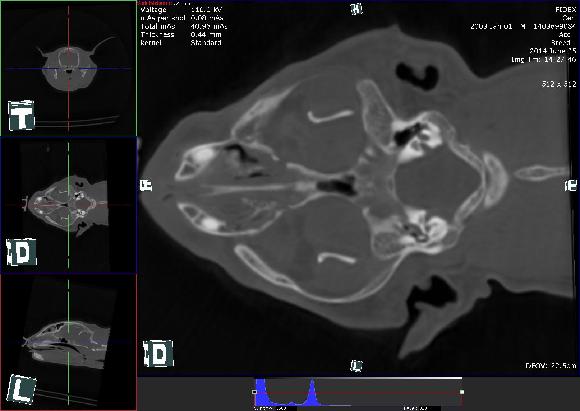
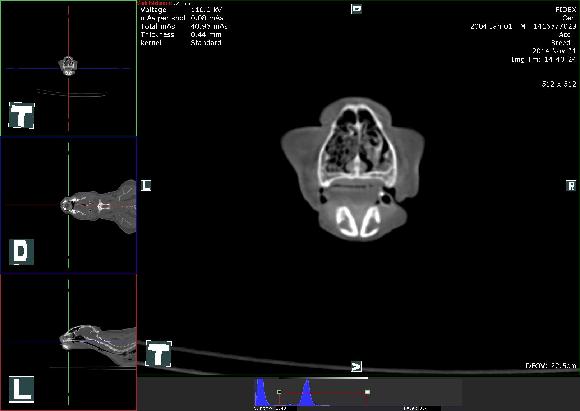
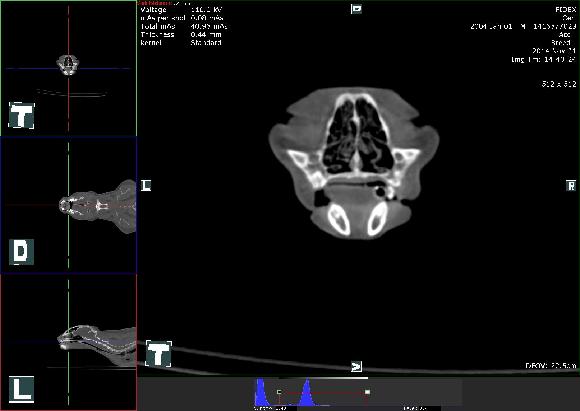
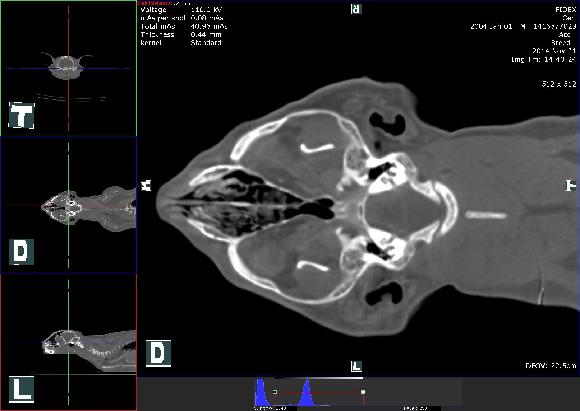
Dr. J. Hnizdo, L.Bicanova - Animal Clinic Bila Hora, Prague Patient: Cat, DSH, female spayed, age: 12 years History: A 12-year-old DSH spayed female cat was evaluated in our clinic because of chronic, progressive inspiratory dyspnea and decreased food intake. No coughing or nasal discharge was observed by the owner. Three years ago this cat and two other cats in the household suffered from herpes virus rhinitis all with succesful recovery. Water intake and behavioral habits seemed to be normal, reported by the owner. Physical examination: Patient was quiet, alert, with a body condition score of 2,5/5. Moderate nasal stridor was present. No abnormalities were noticed during palpation of peripheral lymphonodes. Cardiopulmonary auscultation reveald increased bronchovesicular sounds and an inspiratory wheeze reffered from the upper airways. Othoscopic examination was bilaterally normal. Labwork: A CBC and serum biochemistry were performed and only mild azotemia was observed. 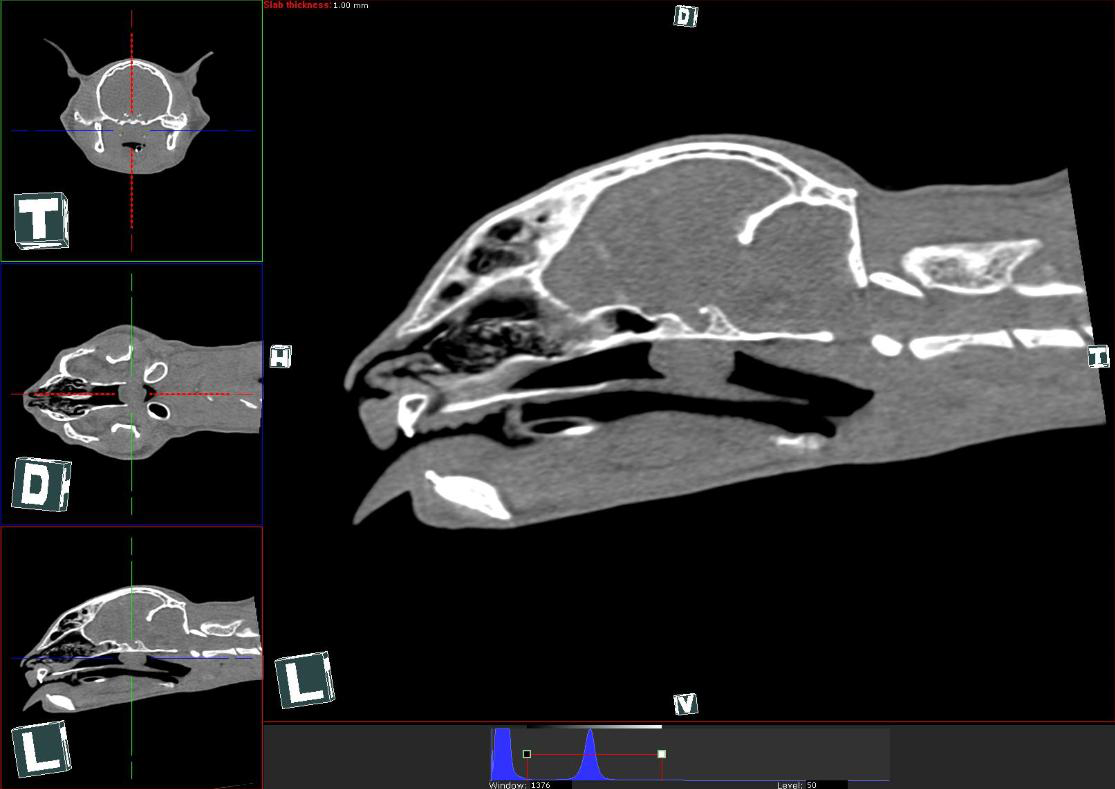 Figure 1. Differential diagnosis:
Treatment: Surgical extitrpation of the mass and histopathologic examination was performed. The right bulla osteotomy with microbiological sampling which was also recommended was declined because of the owners constraints. Final diagnosis: Histologic findings were consistent with malignant lymphoma. Outcome: Chemotherapy or radiation therapy was refused by the owner so we decided to start with Prednisone based treatment. Patient started to eat and breath better. The long term follow-up to this case was unfortunately lost. Comment: Lymphoma (most tumors are feline leukemia virus[FeLV] antigen negative) and epithelial neoplasms (carcinoma, adenocarcinoma, squamous cell carcinoma) are the most common tumors of the feline upper airways. Less frequently reported tumor types include sarcomas, mast cell tumor, melanoma, plasmacytoma, olfactory neuroblastoma, and benign lesions such as hemangioma, chondroma, and neurofibroma.1-3 A tissue sample is required to make a definitive diagnosis of the lesion. Both chronic rhinitis and neoplasia have a high prevalence of aggressive radiographic lesions, including erosion, deviation, and proliferation of bone, and differentiating the two can be difficult.4,5 Recent evaluation of CT imaging in cats with nasal and paranasal disease showed that although certain findings may suggest a CT diagnosis of neoplasia over rhinitis (e.g., osteolysis of paranasal bones, extension of disease into the orbit of facial soft tissues, presence of a space-occupying mass, and turbinate destruction),nasal biopsy is necessary for confirmation.6 CT is not more sensitive than conventional radiography at detecting nasal cavity abnormalities but it is more sensitive at localizing these changes and determining the extent of disease.2 However CT could be very beneficial in nasopharyngeal lesions imaging. Reported cases of upper airway lymphoma treated with radiation or chemotherapy show that survival may be favorable.7 References:
Dachshund with Rear Leg Paralysis and Loss of Bladder Control Summary A Dachshund with rear-leg paralysis and loss of bladder control was tentatively diagnosed with impingement into the spinal canal by a bulging intervertebral disc. A spinal CT scan was done to confirm the diagnosis and spare the patient the additional trauma of an invasive spinal tap/dye study X-ray myelogram. The CT study confirmed and refined the diagnosis, and provided a 3D volume rendering that gave the surgeons a very clear internal map by which to plan the corrective surgery. The surgery was successful and the patient fully recovered. Case Puddle, an 8-year-old Dachshund, presented with paralysis of the hind legs and loss of bladder control. There was no external evidence of trauma. A preliminary diagnosis was made of spinal impingement by intervertebral disc bulge and/or calcification between vertebra T-2 and L-3. Puddle was prepared for a spinal CT scan, including general anesthesia via Propofol. A CT scan was performed (via Fidex, from Animage, LLC). The CT scan MPR images revealed a severe spinal impingement by a bulging/herniated disc with advanced calcification between vertebrae L-3 and L-4 , as well as less dramatic intervertebral disc bulge impingement between adjacent vertebrae. The surgeons reviewed these MPR images, as well as a 3D volume rendering. The volume rendering enabled the surgeons to accurately and quickly map their approach and technique in advance of surgery, saving the patient possible additional surgical trauma. The impingement was corrected surgically and the patient was placed in the recovery ward. Three days later, the patient had regained control of his bladder and was able to walk using his hind legs. A full recovery took place after 14 days. While hind leg/lower body paralysis in Dachshunds is not exactly unusual, and thus not as difficult as some conditions to diagnose, using CT to confirm the diagnosis and locate the injury avoids the need for a spinal tap/dye study X-ray myelogram, and thus avoids this invasive diagnostic study. CT imaging also provides a very clear and unencumbered view of the source and nature of this problem – especially when the cause is subtle in size, shape, and position; as well as provides the surgeon with a preview and clear landmarks that enable the safest and least traumatic surgery possible. 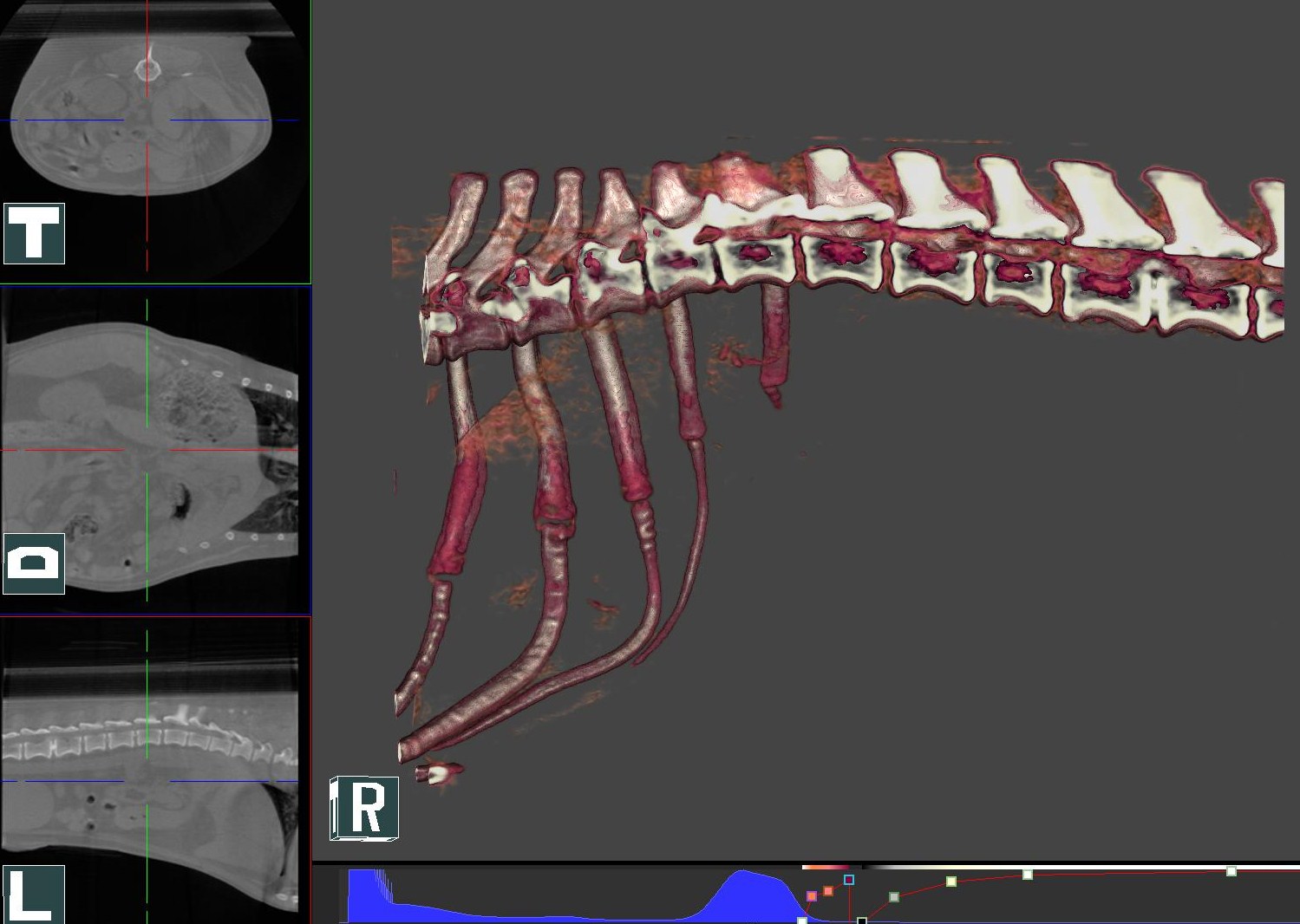 Figure 1: Dachshund Spine (Volume Rendering)
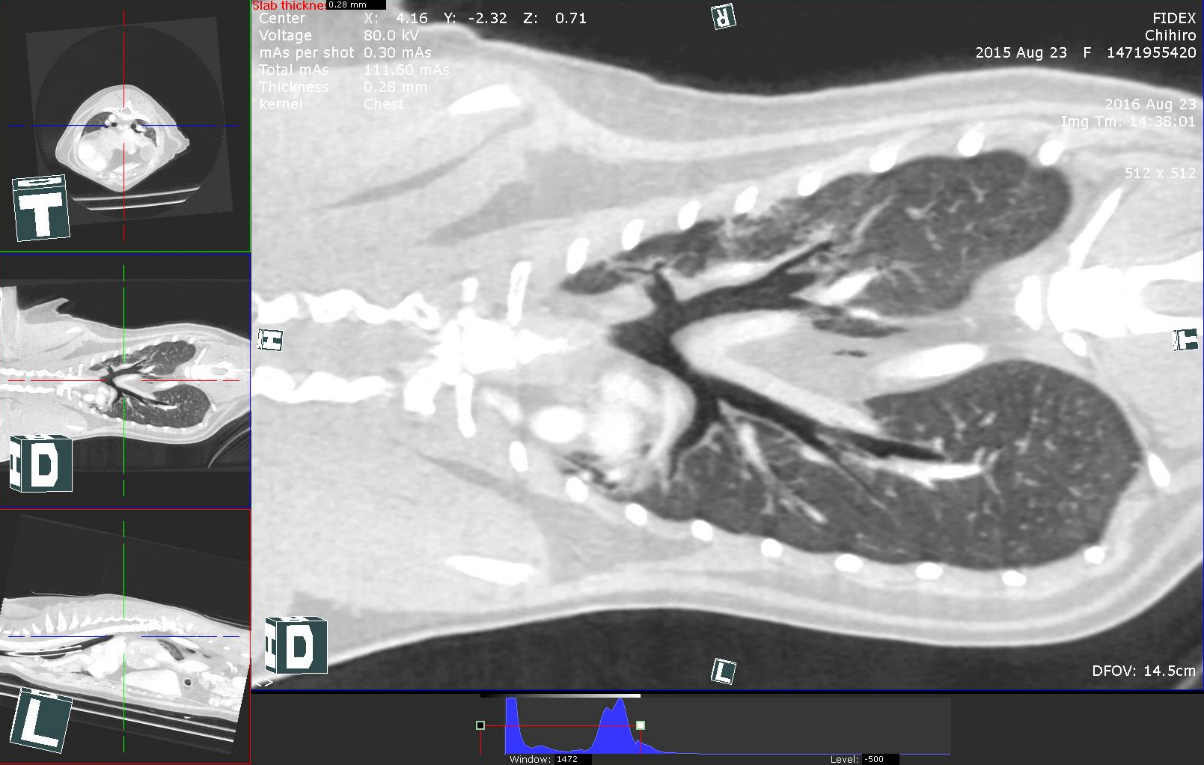
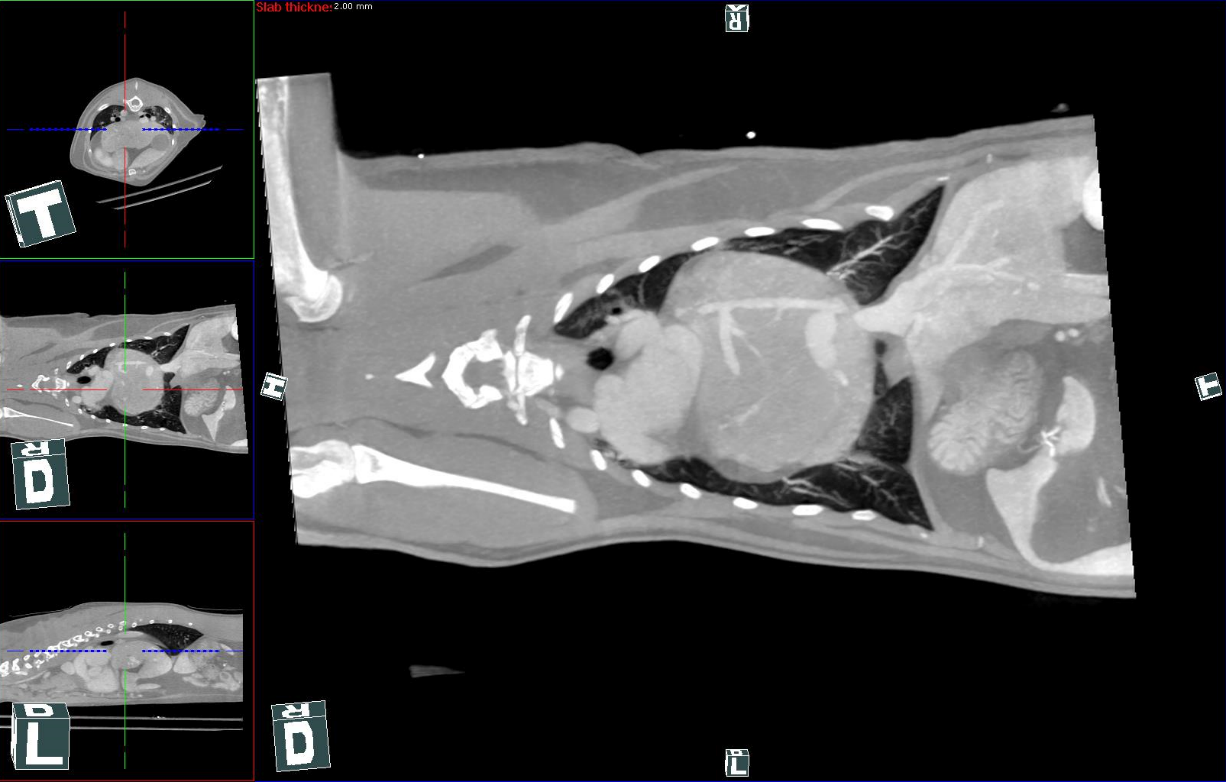
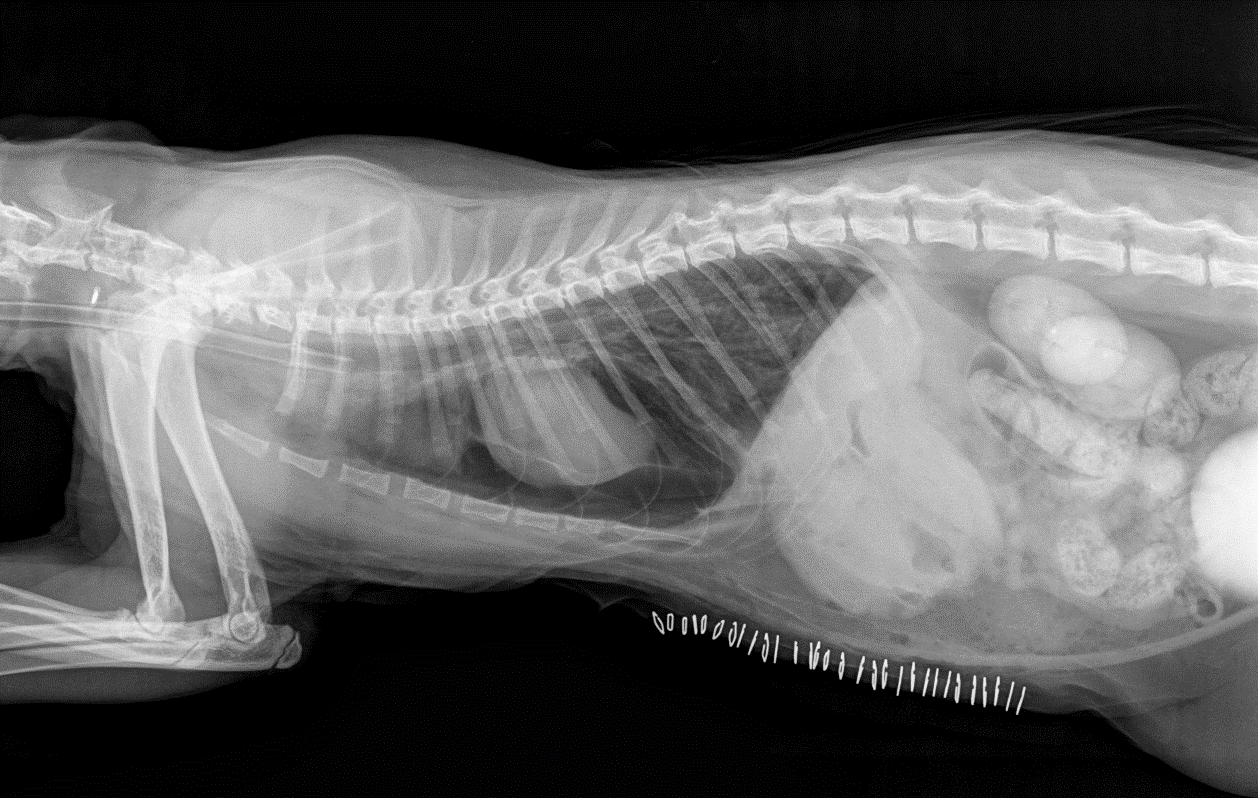
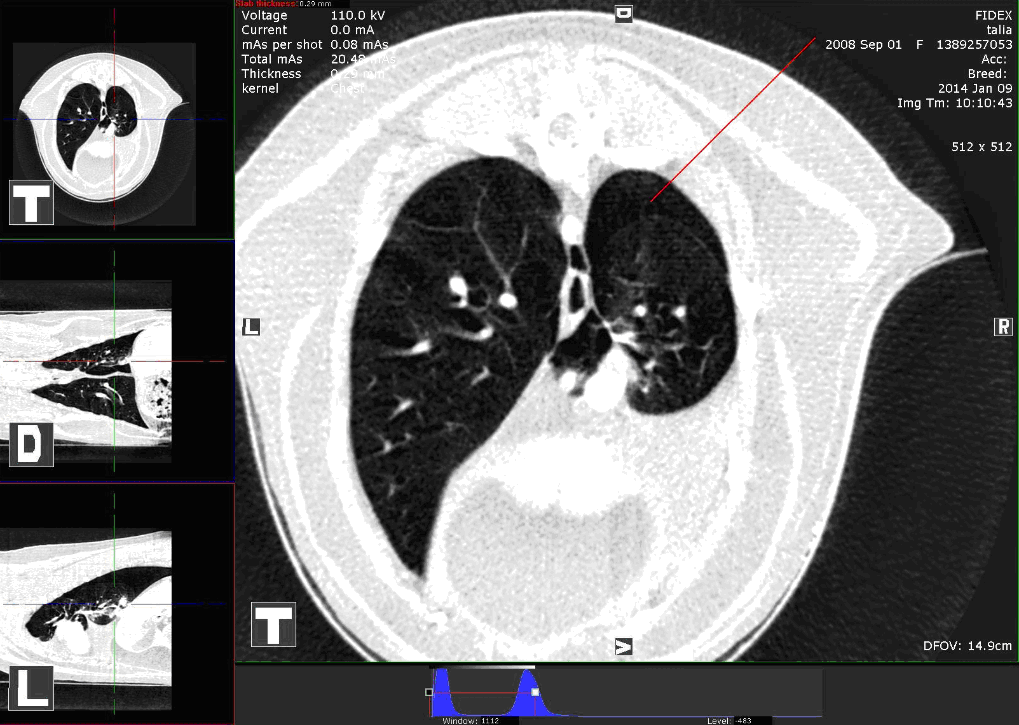
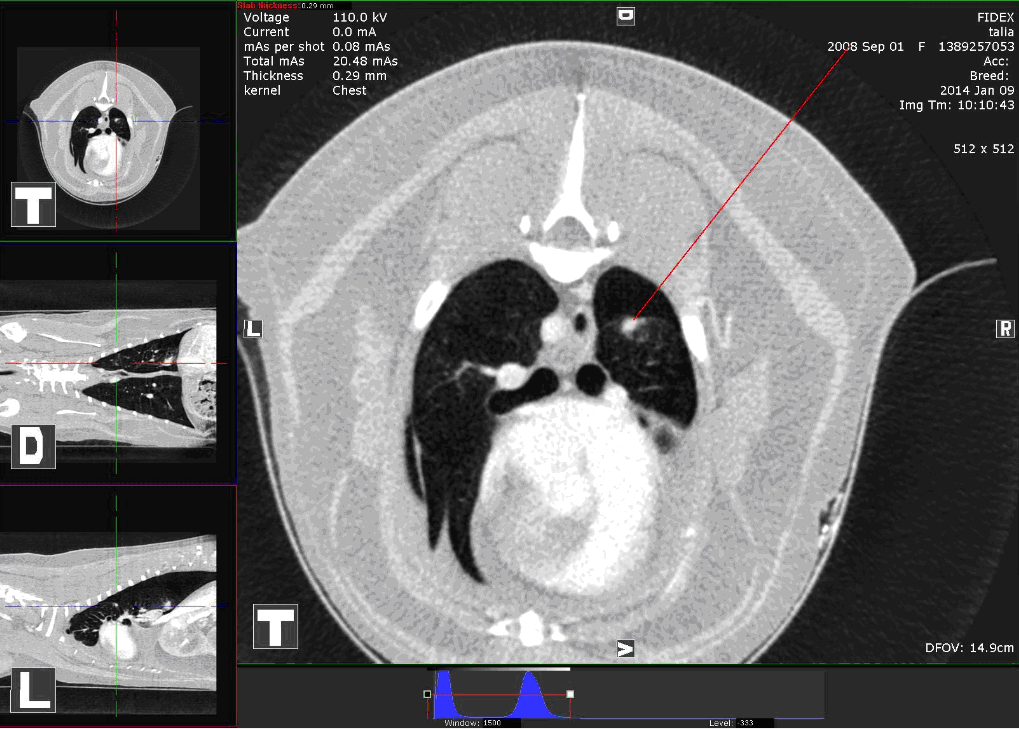
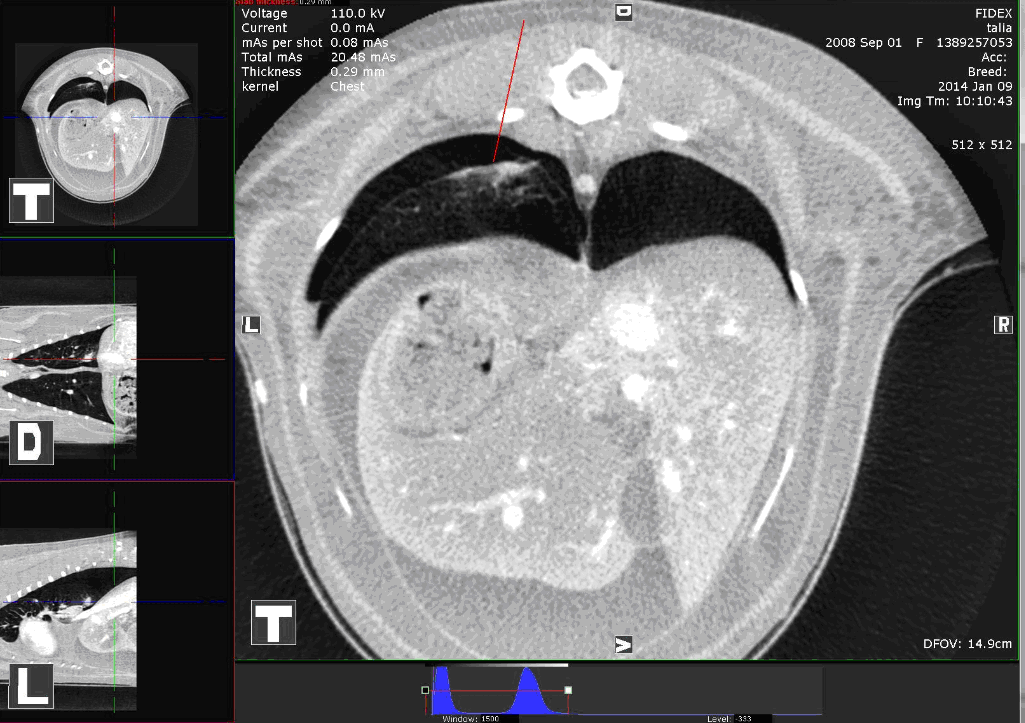
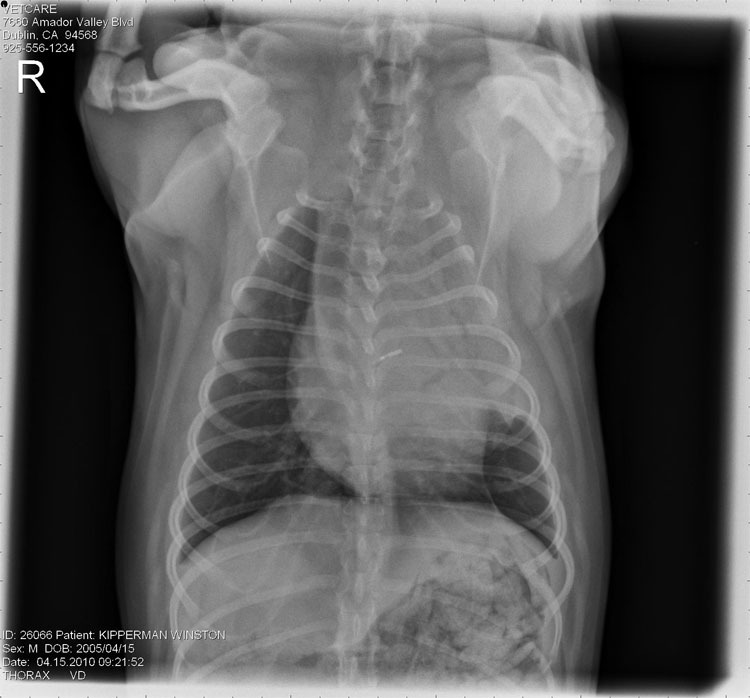
Lung Lobe Torsion in 5-Year-Old Pug Summary A pug dog presenting with acute onset lethargy was tentatively diagnosed with aspiration pneumonia, based on lab work and radiographs. After standard treatment seemed not to have effect, further examination was performed by CT scan via Fidex from Animage, LLC. The CT scan revealed a lung lobe torsion. The patient was treated surgically. The patient then began improving and recovered completely after five days. Case Winston, a 5 year-old, male neutered Pug presented to the Veterinary Emergency and Specialist Center with acute onset lethargy. Physical examination confirmed lethargy and mild fever. Dyspnea was not evident. Lab work revealed an elevated white blood cell count, and radiographs revealed complete consolidation of the left cranial lung lobe with air bronchograms (Figure 1). A tentative diagnosis of aspiration pneumonia was made, and therapy was initiated with IV fluids and broad-spectrum antibiotics. No improvement was noted over the day. Winston was anesthetized with Propofol, and a thoracic CT scan (via Fidex, from Animage, LLC) was performed using a standard breath-hold technique. Pre- and post-contrast images revealed complete consolidation of the left cranial lung lobe with alveolar infiltrates. Air pockets were noted in the central regions of the lobe (Figure 2). The main-stem bronchus to this lobe was constricted at the base and opacified. All other lung lobes appeared normal. CT diagnosis was left cranial lung lobe torsion. The next day a left lateral thoracotomy was performed, with resection of the diseased and infarcted lung lobe. Recovery was uneventful after analgesic support including meloxicam, fentanyl, and local intercostal nerve blocks. Histopathology of the excised lung lobe revealed acute fibrinohemorrhagic necrosis. Winston made a complete recovery by day 5 after surgery. Lung lobe torsion (LLT) is a rare, life-threatening condition in which a lung lobe rotates along its long axis with twisting of the broncho-vascular pedicle.i The cause is unknown. Diagnosis is challenging as LLT is often not suspected until the patient fails to respond to treatment for more common conditions such as pneumonia, and/or pleural effusion occurs. Serial radiographs, thoracic ultrasound and bronchoscopy have been reported as diagnostic aids in past literature.ii A recent report documented a series of 7 Pugs with LLT over a thirteen year period.iii Median age was 1.5 years, and 6 out of 7 cases involved the left cranial lung lobe. In veterinary medicine, CT is being recognized as a valuable tool in clarifying the cause of pulmonary parenchymal diseases. Common CT features of LLT in dogs include pleural effusion, abrupt ending of the affected bronchus, consolidation of the affected lung lobe, and lobar emphysema.iv Winston’s clinical and radiographic findings were suggestive of pneumonia. The decision to pursue CT was based on the absence of any known predisposing factors (vomiting, anesthesia, immuno-suppression) and the known predisposition of young Pugs to develop this disease. In this case, the availability of, and decision to pursue CT imaging early was pivotal in achieving a positive outcome.
i Lord PF, Greiner TP, Greene RW, et al: Lung lobe torsion in the dog. Journal American Animal Hospital Association 1973; 9; 473-482 ii Moon, M, Fossum, TW. Lung lobe torsion. In; Bonagura, JD, ed. Kirk’s Current Veterinary Therapy XII; Small Animal Practice. Philadelphia; WB Saunders Co, 1995; 919-921. iii Murphy, KA, Brisson, BA; Evaluation of lung lobe torsion in Pugs; 7 cases. Journal American Veterinary Medical Association 2006; No 1; 86-90. iv Seiler, G, Schwarz, T, Vignoli, M, Rodriguez, D. Computed tomographic features of lung lobe torsion. Journal of Veterinary Radiology and Ultrasound, Vol 49, No 6, 2008; 504-508.
|
||||||||||||||||||||||||||
| ||||||||||||||||||||||||||